
Male Sexual Dysfunction
"last update: 15 Oct 2024"
- Annexes
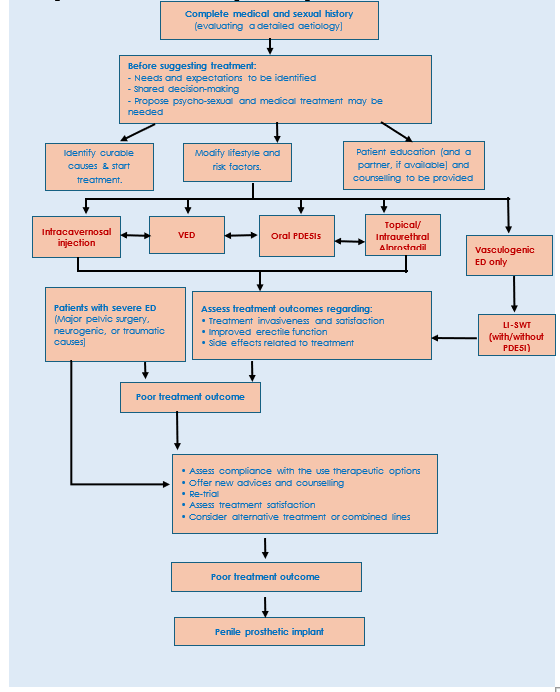
Figure 1: Personalized Management Algorithm:
Figure
2: Management algorithm for
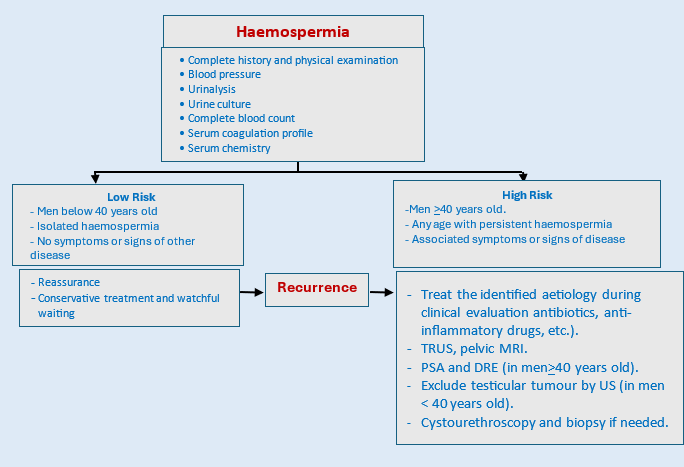
Table 4: Comparison of the properties of phosphodiesterase type 5 inhibitors (PDE5i) (42)
|
Property |
Sildenafil |
Tadalafil |
Vardenafil |
Avanafil |
|
|
TMAX |
30–120min |
30–360min |
30–120min |
30–45min |
|
|
Terminal half life |
4h |
17.5h |
4h |
6–17h |
|
|
Available doses |
25mg,50mg,100mg |
5mg,10mg,20mg |
5mg,10mg,20mg |
50mg,100mh,200mg |
|
|
Max dose |
100mg |
20mg |
20mg |
200mg |
|
|
Efficacy |
Each offer similar efficacy |
||||
|
Side effects (5 most common) |
Headache, flushing, dyspepsia, nasal congestion, alteration in color vision |
Headache, dyspepsia, back pain, myalgia, nasal congestion |
Headache, flushing, rhinitis, dyspepsia, sinusitis |
Headache, flushing, rhinitis, dyspepsia, sinusitis |
|
|
Use with α-blockers.
|
- Concomitant use of selective α-blockers does not present a risk for significant hypotension - There is a risk of significant hypotension when using non-selective α-blockers |
||||
|
Contraindications
|
- Regularly or intermittent use of organic nitrates. - Known hypersensitivity to any component of the tablet |
||||
|
Dose adjustments that may be needed |
· Patients aged > 65 years. · Hepatic impairment · Renal impairment · Concomitant use of potent cytochrome P450 3A4 inhibitors (e.g. ritonavir, cobicistat and erythromycin) · Concomitant use of cimetidine with sildenafil |
||||
|
TMAX = time to maximum plasma concentration. |
|||||
Table 5: Clinical History, Physical Examination, Laboratory Investigations and Radiologic Assessment in Different Types of Priapism (119,120).
|
Variant |
History and clinical examination |
Penile blood appearance |
Penile blood gas findings |
Color Duplex ultrasonography findings |
|
Ischemic priapism |
Tender and rigid corpora cavernosa |
Corpus cavernosum testing: blood is hypoxic and dark in color |
pO2> 30 mmHg pCO2>60 mmHg pH<7.25 |
Minimal or absent blood flow |
|
Nonischemic priapism |
Perineal or penile trauma; non tender, partially tumescent corpora cavernosa |
Corpus cavernosum testing: blood is oxygenated and red |
pO2<90 mmHg pCO2<40 mmHg pH=7.4 similar to normal arterial blood) |
Blood flow is normal to high in velocity |
|
Stuttering (recurrent) priapism |
Similar attacks |
Corpus cavernosum testing: blood is hypoxic and dark in color |
Blood gases: pO2<30 mmHg; pCO2>60 mmHg pH <7.25 |
Minimal or absent blood flow during acute priapism; normal blood flow otherwise |
|
pCO2, partial pressure of carbon dioxide; pO2, partial pressure of oxygen. |
||||
Table 6: Percutaneous distal shunts, open distal shunts, open proximal shunts, and vein anastomoses/shunts
|
Distal shunts |
|
Example |
Technique |
|
Percutaneous distal shunts |
Winter (corporoglanular) |
shunt large biopsy needle is inserted through glans |
|
|
Ebbehoj (corporoglanular) |
shunt #11 blade scalpel is percutaneously passed |
||
|
T shunt (corporoglanular shunt) |
Modified Ebbehoj using #10 blade scalpel and introducing the scalpel rotating it inside 90° |
||
|
Open distal shunt |
Al-Ghorab
|
A 1 cm incision is made distal to coronal sulcus with excision of 5 × 5 mm cone segment of distal tunica albuginea from each corporal body |
|
|
Burnett ‘snake’ maneuver
|
Modification of Al-Ghorab shunt. A Hegar dilator is used to evacuate ischemic blood through a distal tunical window |
||
|
Proximal shunts |
Open proximal shunt |
Quackels or Sacher (corporospongiosal) shunt
|
In lithotomy position, bulbocavernosus muscle is dissected from corpus spongiosum and 1 cm staggered ellipses of tissue are incised/excised from spongiosal/corporal bodies, and the defects anastomosed together |
|
Corporo saphenous vein or superficial/deep dorsal vein shunts |
Grayhack shunt
|
The saphenous vein is ligated and anastomosed with corpora cavernosa |
|
|
Barry shunt
|
The superficial or deep dorsal vein is ligated and anastomosed to the corpora cavernosa |
