
Auditory Brainstem Response (ABR) Testing in Babies
"last update: 26 August 2024"
- Annexes
Editorial Independence:
● This guideline was developed without any external funding.
● All the guideline development group members have declared that they do not have any competing interests.
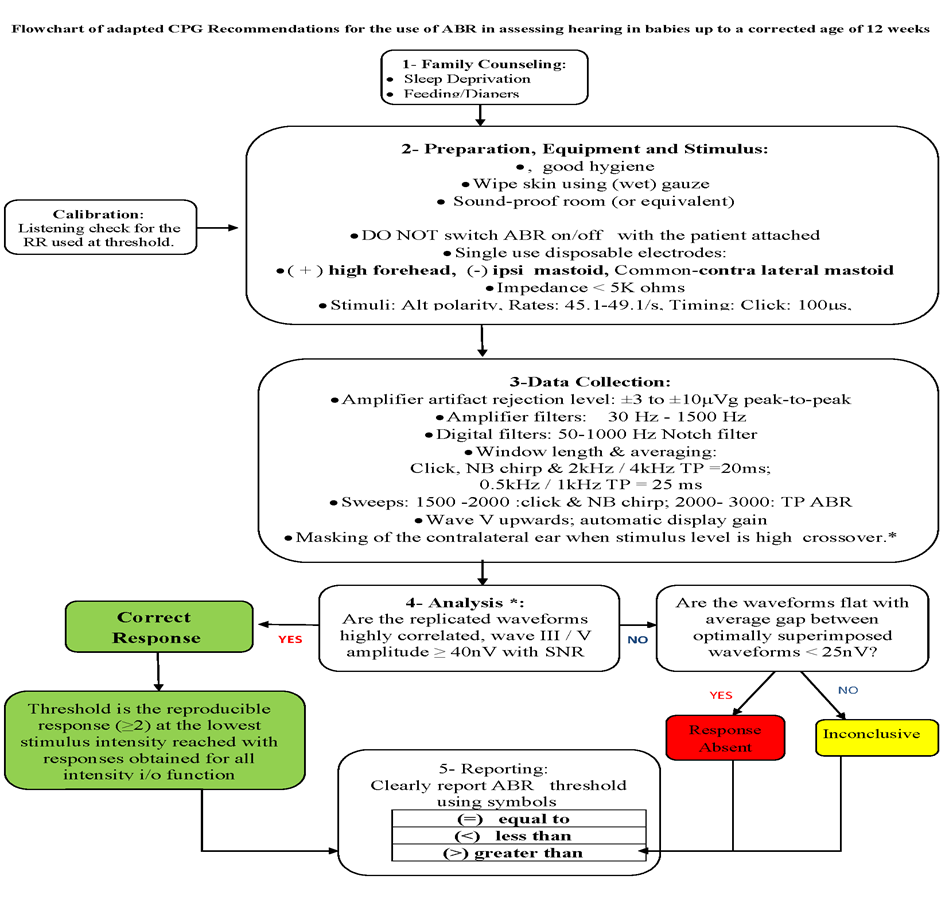
Annex 1: Guideline Flowchart
Annex 2: Tables of appraisal of selected guidelines: Currency (table 1), Content (table 2) and Quality (table 3) of the selected guidelines.
|
No. |
Guideline Name |
Year of Publication |
The Organization |
Age Demography |
|
1 |
Threshold estimation by the tone evoked auditory brainstem response: A literature meta-analysis |
2000 |
Canadian Journal of Speech-Language Pathology and Audiology BY University of British Columbia |
Adult and infant/ child |
|
2 |
Practice guidelines: Principles of external peer review of auditory electrophysiologic measurements |
2018 |
British Society of Audiology |
Newborn |
|
3 |
Guidelines 9C: Recommended standards for Short latency auditory evoked potentials: American neurophysiological guidelines |
2008 |
American Clinical Neurophysiology Society |
Adult, neonates, infants and children |
|
4 |
Recommended Procedure: Auditory Brainstem Response (ABR) Testing in Babies |
2019 |
British Society of Audiology |
Newborn |
|
5 |
Year 2019 Position Statement: Principles And Guidelines For Early Hearing Detection And Intervention Programs |
2019 |
The Joined Committee On Infant Hearing |
Infants |
|
6 |
Guidelines for the early audiological assessment and management of babies referred from the Newborn Hearing Screening Program: Version 3.1 |
2013 |
The UK NHC and NHS screening programs |
Newborns |
Table 2 Content
|
|
Guideline 1 British Columbia 2000 |
Guideline 2 BSA 2018 |
Guideline 3 American Clinical Neurophysiology Society 2008 |
Guideline 4 BSA 2019 |
Guideline 5 JCIH 2019 |
Guideline 6 NHSP 2013 |
|
Credibility |
7 |
8 |
7 |
9 |
8 |
8 |
|
Observability |
7 |
8 |
8 |
9 |
8 |
8 |
|
Relevance |
8 |
6 |
8 |
9 |
8 |
8 |
|
Relative advantage |
8 |
8 |
7 |
9 |
8 |
7 |
|
Easy to install and understand |
7 |
7 |
8 |
9 |
8 |
8 |
|
Compatibility |
7 |
8 |
7 |
9 |
8 |
7 |
|
Testability |
8 |
5 |
7 |
9 |
8 |
8 |
|
Total score |
48 |
50 |
48 |
72 |
64 |
54 |
Table 3 Quality
|
Domain |
Guideline 1 British Columbia 2000 |
Guideline 2 BSA 2018 |
Guideline 3 American Clinical Neurophysiology Society 2008 |
Guideline 4 BSA 2019 |
Guideline 5 JCIH 2019 |
Guideline 6 NHSP 2013 |
|
Transparency |
A |
A |
A |
A |
A |
A |
|
Conflict of interest |
B |
A |
NR |
A |
B |
A |
|
Development group |
A |
A |
B |
A |
A |
A |
|
Systematic review |
A |
B |
C |
A |
A |
A |
|
Grading of evidence |
B |
A |
B |
A |
B |
B |
|
Recommendations |
A |
A |
A |
A |
A |
A |
|
External review |
B |
B |
C |
A |
A |
B |
|
Updating |
C |
A |
C |
A |
A |
B |
Annex 3: The risks and benefits of added and/or modified statements
|
The statement to be adapted: action |
Benefits |
Risk/Harm |
|
Skin should be gently wiped with (wet) gauze , abrasions avoided |
No possibility of skin injury or skin reaction |
No risk or harm |
|
Sleep deprivation, feeding, Diaper change in most situations will lead to natural sleep and lessen activity |
No possible complications from sedatives No special or additional safety precautions needed |
No risk or harm |
|
Thresholds should be measured for at least two frequency audiometric regions: Low frequency thresholds using 0.5khz High frequency thresholds using TP or TB 2 or 4 khz or clicks |
Allows low & high frequency threshold assessment for two region audiometric representation Reduces test time |
No harm
Potential risk of missing mid frequency HL |
|
Criteria for ABR response & threshold: 1-Reproducibilty of at least two response traces: visual and graphic 2-Reproducibility of responses for all intensity i/o function 3-Threshold is the reproducible response at the lowest stimulus intensity reached |
Simplified criteria Matches all response descriptions in the selected guideline Lessens confusion Allows clear , easy & unified reporting of results |
No harm or risk |
|
Clinician listening check for the RR used at threshold. Reference dBSPLpe/ eq if and when feasible |
Psychoacoustic calibration control is feasible and easy and can be routinely done |
No harm or risk |
