Ischemic Stroke
"last update: 9 May 2024"
- Methods
We adopted WHO proposed seven distinct steps for development of clinical guidelines to ensure a thorough and rigorous process.
The final research questions and consensus questions are structured using the ‘Population, Intervention, Control, Outcome’ (PICO) format. Each question is assigned to an appropriate topic group according to the scope.
A literature search is undertaken for each individual question to identify studies that help to answer the question and provide evidence that is robust enough to allow recommendations to be made. Literature searching is coordinated by the stroke guideline team. These initial searches look for guidelines, systematic reviews, and meta-analyses only and cover the following databases:
a. Cochrane Database of Systematic Reviews (CDSR)
b. MEDLINE.
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation. inclusion/exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines Specific range of dates for publication (using Guidelines published or updated 2015 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author not on behalf of an organization in order to be valid and comprehensive, a guideline ideally requires multidisciplinary input.
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in a table:
· Developing organisation/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. The panel decided a cut-off point or rank the guidelines (any guideline scoring above 50% on the rigour dimension was retained). The Guideline Development Group has decided to adapt the current guidelines guided by most recent NICE (2019, reviewed 2022) and AHA/ASA (2019 & 2021) recommendations on ischemic stroke management.
EVIDENCE ASSESSMENT
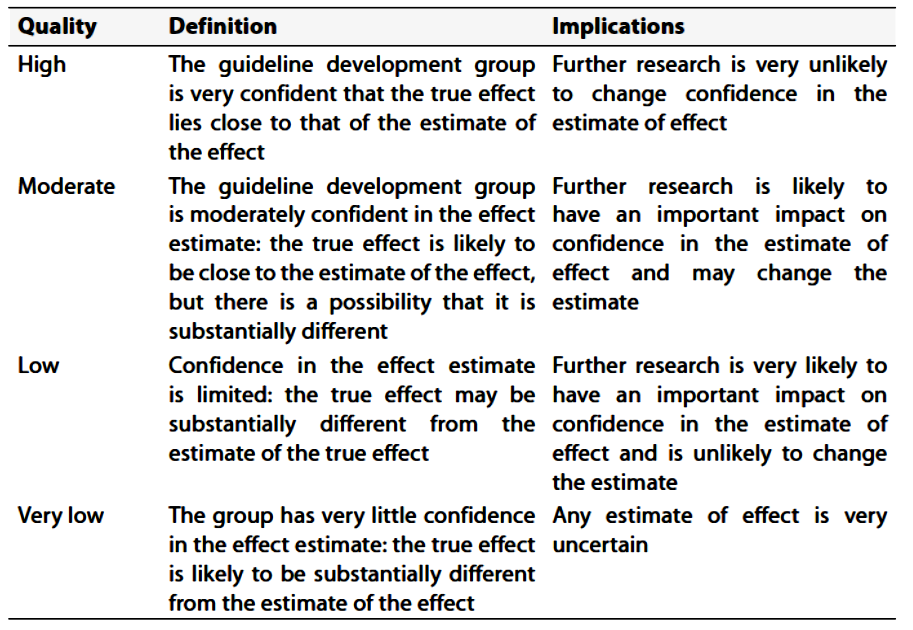
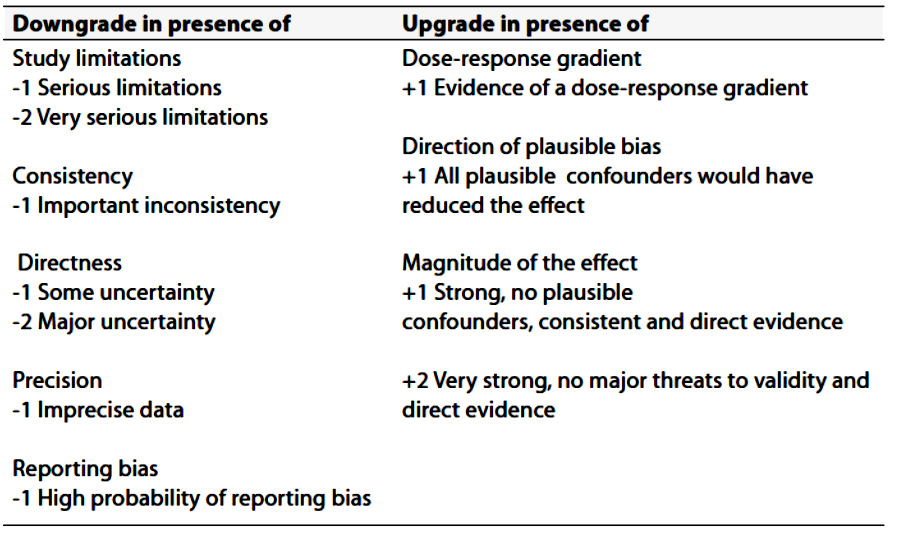
According to WHO handbook for Guidelines we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed information on GRADE is available through the GRC secretariat and on the following sites:
■ GRADE working group: http://www.gradeworkingroup.org
■ GRADE online training modules: http://cebgrade.mcmaster.ca/
■ GRADE profile software: http://ims.cochrane.org/revman/gradepro
THE STRENGTH OF THE RECOMMENDATION
The strength of a recommendation communicates the importance of adherence to the recommendation.
§ Strong Recommandations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
§ Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
§ When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
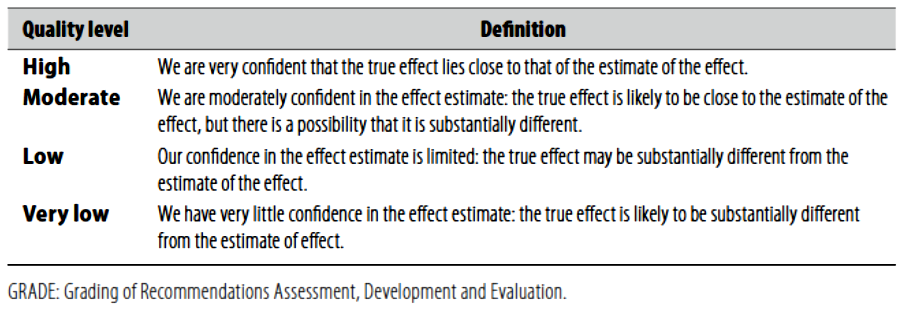
(Table-1) Quality of evidence in GRADE (Table-2) Significance of the four levels
of evidence