
Streptococcosis
"last update: 28 April 2024"
- Diagnosis
a-Clinical sign and lesions
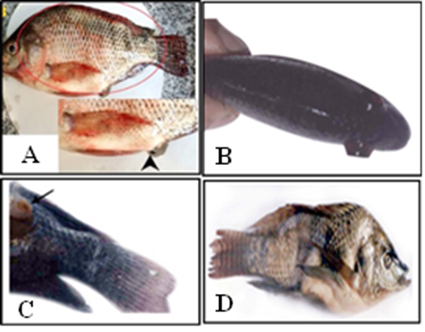
◾The most common clinical signs of streptococcosis are Lethargy, loss of appetite, abnormal behavioral swimming, abdominal distention, severe congestion all over the body, rectal prolapse (Fig 2A), body darkness unilateral or bilateral exophthalmia (Pop eye) (Fig 2B), corneal opacity, abscess like nodule in caudal peduncle and mandible (Fig 2C) and skeletal deformity (Fig 2D) (Abdel-Gawad et al., 2007; El-daim et al., 2023a). Buccal paralysis in the case of S. agalactiae Ib was also observed. Fecal casts or strings are characteristic for streptococcal infection.
◾ Internally, the affected fish may show yellowish to bloody ascitic fluid in the abdominal cavity; pale enlarged liver, dark red spleen; congestion and enlargement of anterior kidneys (El-daim et al., 2023a), fibrinous pericarditis and peritonitis, hemorrhages in the brain, retrobulbar region, intestines, and liver (Sudpraseart et al., 2020).
We should note that these clinical signs are not pathognomonic for streptococcosis because they are not distinct from Lactococcosis caused by L. garvieae & L. piscium, Enterococcosis caused by E. faecalis, Vagococcosis caused by V. salmoninarum.
b-Laboratory diagnosis
Samples: Liver, brain, spleen, and kidneys of affected fish.
I-Presumptive diagnostic assay
Isolation and identification
◾Streptococcous spp are Gram-positive cocci grouped in short to medium-length chains (Fig 3) (Abdel-Gawad et al., 2007), non-motile, catalase negative, oxidase negative, fermentative, with a negative VP response.◾ On 5% sheep blood agar, tryptic soy agar, and brain heart infusion agar incubated at 25 to 35oC for 24 to 48 hrs, small white and umbonate colonies (up to 1 mm) with an entire opaque border are produced.
◾ Strept. dysgalactiae on Colombia blood agar (CBA) demonstrated the presence of pinpoint white colonies (0.5 mm) (Yang and Li, 2009).
◾ RAPID Strep strip, VITEX systems, API 20E STREP, Rapid Strep 32 and ATB Expression System can be carried out, however, incomplete, or incorrect pathogen database may result in improper identification of bacteria.
II-Histopathological examination
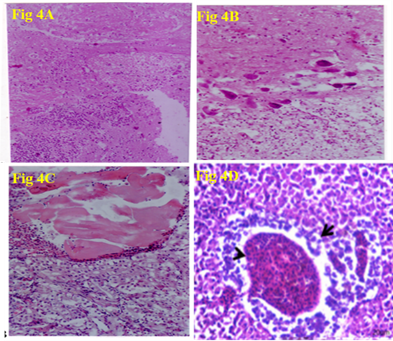
◾ Congestion of the cerebral blood vessels together with focal areas of encephalomalacia (Fig 4A), Galiosis, satillitosis, neural degeneration and neurophagia (Fig 4B), Abscess formation characterized by areas of necrosis surrounded by inflammatory cells was observed in kidneys (Fig 4C) were recorded in Nile tilapia infected with Streptococcous sp (Abdel-Gawad et al., 2007). Liver of Nile tilapia infected with Streptococcus agalactiae revealed dilated hepatic blood vessels (arrowheads), degenerative and necrotic changes of pancreatic epithelium (Fig 4D) (El-daim et al., 2023a).
III-Confirmatory diagnosis
Serological identification
◾Lancefield grouping (A-H and K-V) described serological identification of hemolytic and non-hemolytic bacteria based on group-specific polysaccharides (C antigen). Serological tests, such as the enzyme-linked immunosorbent assay indirect fluorescent antibody are applied for quick detection and identification of bacteria. (Huang et al., 2018).
◾ Strept. iniae and Strept. ictaluri are non-groupable with the Lancefield method (Shoemaker et al. 2017).
Molecular identification
◾ PCR diagnosis of various Streptococcus spp based on the selective amplification of the 16S rRNA, 16S-23S rRNA gene, heat-shock genes (groESL), and tRNA gene intergenic spacer regions (ITSs) is used for confirmative identification (Ortega et al., 2018).
◾ Loop-mediated isothermal amplification method (LAMP) (Wang et al., 2012); Multi Locus Sequence Typing (MLST) (Heckman et al., 2020), and MALDI-TOF-MS (Souter et al., 2021)
