Tympanometry
| Site: | EHC | Egyptian Health Council |
| Course: | Otorhinolaryngology, Audiovestibular & Phoniatrics Guidelines |
| Book: | Tympanometry |
| Printed by: | Guest user |
| Date: | Monday, 23 December 2024, 10:02 PM |
Description
"last update: 5 August 2024"
- Acknowledgements
Chief Editor: Reda Kamel1
General Secretary: Ahmed Ragab2
General Coordinator: Baliegh Hamdy3
Scientific Board: Ashraf Khaled,4 Mohamed Ghonaim,5 Mahmoud Abdel Aziz,6 Tarek Ghanoum,7 Mahmoud Yousef8
Audiology Executive Manager: Iman El-Danasoury9 Assembly board: Enaas Kolkaila,10 Mostafa Elrefaie10 Grading Board (In alphabetical order)
Mohamed Abdelghaffar,11 Rafeek Mohamed Abdelkader,12 Abeir Dabbous,7 Iman El Adawi,13 Mona El Akkad,14 Mohamed El-Badry,12 Iman El-Danasoury,9 Tarek ElDessouky,15 Wafaa El Kholi,9 Trandil El Mehallawi,10 Reham Elshafei,14 Amira El Shennawy,7 Enaas Hassan,16 Nagwa Hazzaa,9 Naema Ismail,13 Nadia Kamal,9 Rabab Koura,15 Radwa Mahmoud,17 Salwa Mahmoud,18 Soha Mekki,19 Iman Mostafa,15 Mona Mourad,20 Nashwa Nada,10 Abir Omara,18 Mohamed Salama16
Hesham Sami,12 Hesham Taha,9 Somia Tawfik9
Reviewing Board: Hesham Kozou,20 Rasha Elkabarity,9 Hosam Sanyelbhaa21
1Otorhinolaryngology Department, Faculty of Medicine/ Cairo University, 2Otorhinolaryngology Department, Faculty of Medicine/ Menoufia University, 3Otorhinolaryngology Department, Faculty of Medicine/ Minia University, 4Otorhinolaryngology Department, Faculty of Medicine/Beni-Suef University, 5Otorhinolaryngology Department, Faculty of Medicine/Mansoura University, 6Otorhinolaryngology Department, Faculty of Medicine/ Tanta University, 7Audiovestibular Unit, Otorhinolaryngology Dep. Faculty of Medicine/ Cairo University, 8Phoniatrics Unit, Otorhinolaryngology Department, Faculty of Medicine/ Ain Shams University, 9Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Ain Shams University, 10Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Tanta University, 11Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Sohag University, 12Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Minia University, 13Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Al Azhar University,14Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Fayoum University, 15Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Tanta University,16 Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Assiut University, 17Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Banha University,18Audiovestibular Unit, Otorhinolaryngology Department/ Hearing and Speech Institute, 19Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Zagazig University, 20Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Alexandria University, 21Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Menoufia University.
Sincere thanks extend to the secretaries: Samar Hussein and Eman Ragab, as well as the editor: Mohamed Salah
- Abbreviations
AAA Americam Academy of Audiology
BSA British Society of Audiology
- Executive Summary
The tympanometer and probe
tip shall be clean (i.e. free from dust and dirt and in compliance with local
infection control standards).
Tympanometers shall meet the performance and calibration requirements of
BS EN 60645–5. (strong recommendation).
Calibration: The calibration of the instrument shall
be checked daily with the probe fitted to an appropriate cavity such as the one
supplied by the manufacturer. (strong recommendation).
The subject should be
seated comfortably and should remain as still as possible during the test.
(strong recommendation)
Young children may need to
be held by an appropriate adult, which should be the person responsible for the
child. (conditional recommendation)
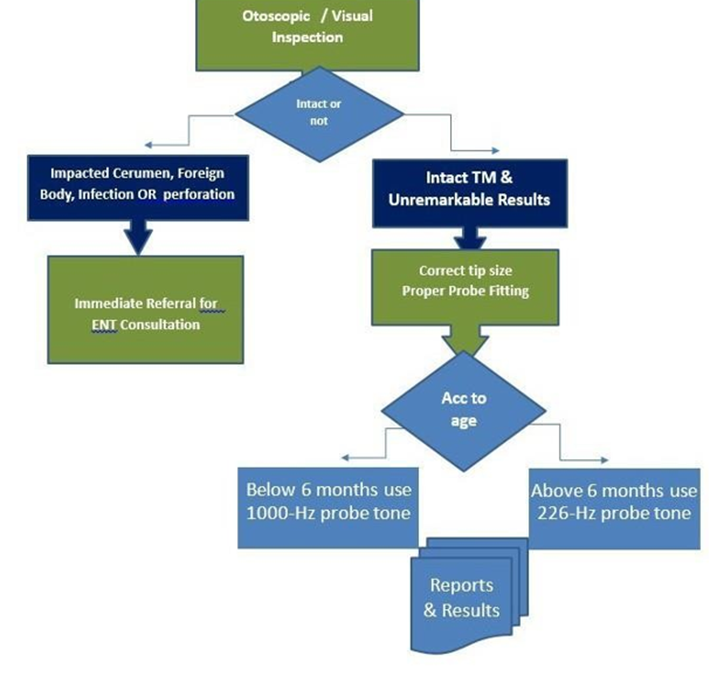
Tympanometry shall be preceded by otoscopic examination to ensure that there are no contraindications to continue. (strong recommendation)
Testing shall proceed only with informed consent (e.g. verbally) from the subject or person responsible for the subject and if it is the judgement of the tester that it is safe to do so. (conditional recommendation)
Subjects with age over 6 months, using a 226-Hz probe tone is recommended (Strong recommendation)
Subjects with a corrected age under 6 months using a 1000-Hz probe tone. (strong recommendation)
Tympanometric results do not identify pathology uniquely and should be interpreted in the context of other information from the complete test battery being conducted and with particular regard to the otoscopic findings and history. (Strong recommendation)- Introduction, purpose, scope and audience
Introduction:
Scope:
The recommendations are deemed suitable for routine clinical measurements applicable to most types of instruments measuring aural acoustic impedance/ admittance using a nominal probe frequency of 226 Hz for subjects whose corrected age is equal to or greater than 6 months (i.e. at least 6 months from the child’s due date), and 1000 Hz for subjects below 6 months corrected age.
Target audience:
Audiovestibular physicians
- Methods
Methods of development
Stakeholder Involvement: Individuals who were involved in the development process. Included the above-mentioned Audiology Chief Manager, Audiology Executive Manager, Assembly Board, Grading Board and Reviewing Board.
Information about target population experiences were not applicable for this topic.
Search Method
Electronic database searched:
Eg: Pubmed, Medline, Egyptian Knowledge Bank, Medscape, WebMD, Google Scholar
Keywords
Tympanometry – impedance – ear drum
The adaptation cycle passed over: set-up phase, adaptation phase (Search and screen, assessment: currency, content, quality & /decision/selection) and finalization phase that included revision and external reviewing.
Time period searched: from August 2012 to 2018
Results
Three guidelines were assessed by two audiovestibular medicine experts and the British Society of Audiology, Recommended Procedure: Tympanometry, published in 2013 and reviewed in 2018, had the highest scores as regards to the currency, contents and quality. It was graded by 30 audiovestibular medicine consultants and reviewed by three expert reviewers.
Setting: Primary, secondary and tertiary care centers & hospitals, and related specialties.
Interpretation of strong and conditional recommendations for an intervention
|
Audience |
Strong recommendation |
Conditional recommendation |
|
Patients |
Most individuals in this situation would want the recommended course of action; only a small proportion would not. Formal decision aides are not likely to be needed to help individuals make decisions consistent with their values and preferences. |
Most individuals in this situation would want the suggested course of action, but many would not |
|
Clinicians |
Most individuals should receive the intervention. Adherence to the recommendation could be used as a quality criterion or performance indicator. |
Different choices will be appropriate for individual patients, who will require assistance in arriving at a management decision consistent with his or her values and preferences. Decision aides may be useful in helping individuals make decisions consistent with their values and preferences. |
|
Policymakers |
The recommendation can be adopted as policy in most situations. |
Policy-making will require substantial debate and involvement of various stakeholders. |
WHO handbook for guideline development – 2nd ed.
Chapter 10, page 129
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to Decision frameworks (GRADE Working Group 2013)
|
Grade |
Definition |
|
High
|
We are very confident that the true effect lies close to that of the estimate of the effect. |
|
Moderate
|
We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different |
|
Low
|
Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. |
|
Very Low
|
We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect |
- Recommendations
The following statements and flowchart were adapted from the Guidelines from the British Society of Audiology, Recommended Procedure: Tympanometry, published in 2013 and reviewed in 2018 which received the highest scores as regards the currency, contents, and quality.
Recommendations statements

|
Statement topic |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
reference |
|
1.Equipment
|
1.1. The tympanometer and probe tip shall be clean (i.e. free from dust and dirt and in compliance with local infection control standards). Tympanometers shall meet the performance and calibration requirements of BS EN 60645–5. |
Very low |
Strong |
Expert opinion |
2,3,4 |
|
1.2. Calibration:
The calibration of the instrument shall be checked daily with the probe
fitted to an appropriate cavity such as the
one supplied by the manufacturer. The performance of the instrument shall also be checked on an ear known to produce a normal, peaked tympanogram
(e.g. to ensure the pump is operational and its
tube is not blocked). |
Very low |
Strong |
Expert opinion |
2,3,4 |
|
|
2.Subject prepa- ration
|
2.1. Before examination, the subject (or the person responsible for the subject) should be asked if he/she currently has any ear-related symptoms (including discomfort, pain and discharge), is currently being treated for any ear-related problems or has previously had surgery involving the ears. |
Very low |
Conditional |
Expert opinion |
2,3 |
|
2.2. The subject should be seated comfortably and should remain as still as possible during the test. |
Very low |
Strong |
Expert
opinion |
2, 5,6 |
|
|
2.5. Young children may need to be held
by an appropriate adult, which should be the person
responsible for the child. |
low |
Conditional |
Observational study |
7 |
|
|
3.Otoscopic ex- amination |
3.1. Tympanometry should be preceded by otoscopic examination to ensure that there are no contraindications to continue. Otoscopy in neonates is only intended as a general inspection of the outer ear for obvious signs of disease, blockage or malformation. |
low |
Strong |
Observational validation study |
2,8 |
|
4.Informed con- sent
|
4.1. Testing should proceed only with informed consent (e.g. verbally) from the subject or person responsible for the subject and if it is the judgement of the tester that it is safe to do so. |
Very low |
Conditional |
Expert opinion |
2,5 |
|
5.Subject instruc- tions
|
5.1. The examiner should explain, and where necessary demonstrate, the procedure to the subject and/or person responsible for the subject. |
Very low |
Conditional |
Expert opinion |
2,5 |





|
6.Test procedures
|
6.1 Subjects with age over 6 months, using a 226-Hz probe tone is recommended: • Fit a clean tip of suitable size and shape to the probe and straighten the ear canal by gently pulling the pinna. • Point the probe in the direction of the tympanic membrane to avoid the risk of occluding the probe aperture, for example against the wall of the canal. • A slow rate of change of pressure (50 daPa s–1 or less) should be used but with young children it may be beneficial to use a faster sweep, sacrificing some accuracy for speed of operation. • In the absence of other requirements, tracking should commence at +200 daPa and end once the peak, if it exists, has been clearly recorded. • On automatic systems a lower limit of about –300 daPa, depending on instrument, should normally be selected but occasionally it may be necessary to go to –600 daPa in search of a peak. • In cases of normal tympanograms, tracking should stop at –200 daPa for adults and –300 daPa for children to minimise discomfort. • When testing adults and children on the same equipment, all test parameters should be checked and set appropriately prior to testing. • If an unexpected result is obtained the test should be repeated in its entirety, that is, by removing the probe, inspecting the ear, checking the probe to ensure it is not blocked, for example with wax, and re-testing. • Unexpected results should not be accepted without verifying that they are repeatable and running a calibration check of the probe in the test cavity and performing biologic calibration. • After tympanometry has been completed the probe tip should be removed and all contaminated tips shall be disposed of or cleaned as per local policy. |
Very low |
Strong |
Expert opinion |
2, 9 |

|
|
6.2 Subjects with a corrected age under 6 months using a 1000-Hz probe tone • Fit a clean tip of suitable size and shape to the probe and straighten the ear canal (e.g. by gently pulling the pinna downwards and outwards). • Point the probe in the direction of the tympanic membrane to avoid the risk of sealing the tip against the wall of the canal. • Movement of the infant and crying can result in a false peak in the tympanogram. The baby does not need to be asleep but should definitely be resting quietly during the test. • The direction of pressure change should be from positive to negative and the range should be at least from +200 daPa to –400 daPa (and preferably– 600daPa). • A fast screening mode speed of up to 600daPa s–1 should be used. • Traces should usually be repeated, if possible, to check that the result is repeatable and not due to artefacts such as baby movement. It is especially important to retest any ear with an abnormal or difficult-to-interpret tympanogram. • After tympanometry has been completed the probe tip shall be removed and all contaminated tips shall be disposed of or cleaned as per local policy. |
low |
Strong |
Observational study |
2,9,10 |
|
7.Results and reporting
|
7.1.Tympanometric results do not identify pathology uniquely and should be interpreted in the context of other information from the complete test battery being conducted and with particular regard to the otoscopic findings and history. |
low |
Strong |
Observational study
|
2, 11 |

- Monitoring and evaluating the impact of the guideline
Monitoring/ Auditing Criteria
The audiovestibular physicians should:
▶️Ensure that the tympanometers meeting the performance and calibration requirements of of BS EN 60645–5.
▶️Calibrate the instrument daily.
▶️ Proper history taking for exclusion of any ear-related symptoms.
▶️ Otoscopically examine the ear and obseve the outer ear signs of disease, blockage or malformation.
▶️ Ensuring that the informed consent preceding the test.
▶️ Test the Subjects with age over 6 months, using a 226-Hz probe tone.
▶️ Test the Subjects with a corrected age under 6 months using a 1000-Hz probe tone.
▶️ Be able to interpret the results with other information obtained from the other complete test battery and patient history.
- Updating of the guideline
Updating Procedure:
Any recommendation of this guideline will be updated when new evidence that could potentially impact the current evidence base for this recommendation is identified. If no new reports or information are identified for a particular recommendation, the recommendation will be revalidated. The focus will be on recommendations supported by very-low- or low certainty evidence and where new recommendations or a change in the published recommendations may be needed.
- References
1.Mona M., Jack Roush, Judith Gravel, et al. Audiologic Guidelines for the Assessment of Hearing in Infants and Young Children. August, 2012.
2. Recommended Procedure: Tympanometry, British Society of Audiology. Berkshire (United Kingdom): British Society of Audiology, 2-20. 2013. Reviewed in 2018.
3. American Speech-Language-Hearing Association (1988) Tympanometry. http://www.asha.org/policy/RP1988-00027.htm (accessed 17th July 2013).
4. Electroacoustics - audiometric equipment - part 5: Instruments for the measurement of aural acoustic impedance/admittance (2005) ComplianceOnline. Available at: https://www.complianceonline.com/electroacoustics-audiometric-equipment-part-5-instruments-for-the-measurement-of-aural-acoustic-impedance-admittance-standards-824919-prdp (Accessed: 28 April 2024).
5. American Academy of Audiology, evidence based best practice (AAA). (n.d.). American Academy of Audiology website.
6. British Society of Audiology (2003) Procedure for Processing Documents. Reading: British Society of Audiology.
7. Baldwin M (2006) Choice of probe tone and classification of trace patterns in tympanometry undertaken in early infancy. Int J Audiol 45: 417–427.
8. Eliachar I, Northern JL (1974) Studies in tympanometry: validation of the present technique for determining intra-tympanic pressures through the intact eardrum. Laryngoscope 84: 247–255.
9. British Society of Audiology (2010) Recommended Procedure for Ear Examination. Reading: British Society of Audiology.
10. Marchant CD, McMillan PM, Shurin PA, Johnson CE, Turczyk VA, Feinstein JC, Panek DM (1986) Objective diagnosis of otitis media in early infancy by tympanometry and ipsilateral acoustic reflexes. J Pediatr 109: 590–595
11. Renvall U, Holmquist J (1976) Tympanometry revealing middle ear pathology. Ann Otol Rhinol Laryngol 85: 209–215.
- Annexes
Editorial Independence:
▶️ This guideline was developed without any external funding.
▶️ All the guideline development group members have declared that they do not have any competing interests.
Annex 1: Guideline Flowchart
Annex 2: Tables of appraisal of selected guidelines: Currency (table 1), Content (table 2) and Quality (table 3) of the selected guidelines.
|
No. |
Guideline name |
Year of publication |
The organization |
Age demography |
|
1 |
British Society of Audiology, recommended procedure |
2013 |
British Society of audiology |
Children and adults |
|
2 |
Audiologic guidelines for the Assessment of hearing in infants and young children |
2012 |
AAA |
Infants and Children |
|
3 |
British Society of Audiology, recommended procedure |
2018 |
British Society of audiology |
Children and adults |
|
4 |
Canadian CPGs |
2018 |
College of Audiologists and Speech-Language Pathologists of Ontario |
Adults |
2. Assessment of
Content Table:
|
Criteria |
Guideline A Audiologic Guidelines for the Assess. of Hearing in Infants &Young Children 2012 |
Guideline B British Society of Audiology, Recommended Procedure 2013 |
Guideline C British Society of Audiology, Recommended Procedure 2018
|
Guideline D College of Audiologists and Speech-Language Pathologists of Ontario 2018 |
|
Credibility |
8 |
8 |
8 |
5 |
|
Observability |
7 |
7 |
8 |
7 |
|
Relevance |
6 |
8 |
8 |
6 |
|
Relative Advantage |
8 |
8 |
8 |
4 |
|
Easy to install and understand |
6 |
8 |
8 |
4 |
|
Compatibility |
7 |
8 |
8 |
4 |
|
Testability
|
8 |
8 |
8 |
5 |
|
Total |
50 |
55 |
56 |
35 |
3. Assessment of Quality:
|
|
British Society of Audiology, Recommended Procedure BSA, 2013
|
Audiologic Guidelines for the Assessment of Hearing in Infants and Young Children August 2012 |
British Society of Audiology, Recommended Procedure BSA 2018 |
College of Audiologists and Speech-Language Pathologists of Ontario, 2018
|
|
Transparency
|
A |
C |
A |
A |
|
Conflict of interest
|
A |
NR |
A |
A |
|
Guideline development |
B |
C |
B |
B |
|
Systematic review
|
A |
B |
A |
A |
|
Recommendations |
A |
B |
A |
A |
|
Grading of evidence |
A |
A |
A |
B |
|
External review
|
A |
NR |
A |
B |
|
Update |
A |
C |
A |
B |
4. Comparison table between selected guidelines:
|
|
British Society of Audiology, Recommended Procedure BSA, 2013
|
Audiologic Guidelines for the Assessment of Hearing in Infants and Young Children August 2012 |
British Society of Audiology, Recommended Procedure BSA 2018 |
College of Audiologists and Speech-Language Pathologists of Ontario, 2018
|
|
Credibility |
Documented with evidence based practice |
With evidence based practice |
Documented with evidence based practice |
Not documented |
|
Observality |
Used, practiced and was revised |
not revised |
Used, practiced and was revised |
Used, practiced and was revised |
|
Relevance |
Addresses a sharply problem |
Addresses a sharply problem |
Addresses a sharply problem |
It doesn't address a sharply problem |
|
Relative Advantage |
It's practice offers benefits over the existing practice |
It's practice offers benefits over the existing practice |
It's practice offers benefits over the existing practice |
It's practice doesn't offer benefits over the existing practice |
|
Easy to install and understand |
It is easy to install and to be understood |
It is easy to install and to be understood |
It is easy to install and to be understood |
It is not easy to install and to be understood |
|
Compatibility |
It's practice fits well with our national practice |
It's practice fits well with our national practice |
It's practice fits well with our national practice |
It's practice doesn’t fit well with our national practice |
|
Testibility |
It was tested since it was revised |
It wasn't tested since it was revised |
It was tested since it was revised |
It wasn't tested since it was revised |