PHONIATRICS Learning disability CORRECTED
| Site: | EHC | Egyptian Health Council |
| Course: | Otorhinolaryngology, Audiovestibular & Phoniatrics Guidelines |
| Book: | PHONIATRICS Learning disability CORRECTED |
| Printed by: | Guest user |
| Date: | Monday, 23 December 2024, 10:20 PM |
Description
"last update: 10 June 2024"
- Acknowledgements
Chief Editor: Reda Kamel1
General Secretary: Ahmed Ragab2
General Coordinator: Baliegh Hamdy3
Scientific Board: Ashraf Khaled,4 Mohamed Ghonaim,5 Mahmoud Abdel Aziz,6 Tarek Ghanoum,7 Mahmoud Yousef8
Phoniatrics Chief Manager: Mahmoud Youssef8
Phoniatrics Executive Manager: Dalia Mostafa9
Assembly Board: Safaa Refaat El-Sady,8Azza Abdel-Aziz Azzam,10Omayma Elsayed Afsah,11Aisha Fawzy AbdelHady9
Grading Board (In alphabetical order)
Ahmed Ali,12AhlamA.N.El-Adawy,13Iman ElRouby,10Dalia Mostafa Osman,9Rasha Farouk Safwat,9Yossra Abdel Naby Sallam,14Aya Sheikhany9
Reviewing Board: Sahar Saad Shohdi, 9Sabah Hassan,8Fatema Kaddah8, Reham Mohamed Kamel,15
1Otorhinolaryngology Department, Faculty of Medicine/ Cairo University, 2Otorhinolaryngology Department, Faculty of Medicine/Menoufia University,3Otorhinolaryngology Department ,Faculty of Medicine/Minia University,4Otorhinolaryngology Department ,Faculty of Medicine/Beni-Suef University,5Otorhinolaryngology Department ,Faculty of Medicine/Tanta University,
6Otorhinolaryngology Department, Faculty of Medicine/ Mansoura University, 7Audio vestibular Unit, Otorhinolaryngology Department ,Faculty of Medicine/Cairo University,8Phoniatrics Unit, Otorhinolaryngology Department, Faculty of Medicine/ Ain Shams University, 9Phoniatrics Unit, Otorhinolaryngology Department, Faculty fMedicine/ Cairo University, 10Phoniatrics Unit, Otorhinolaryngology Department/Hearing and Speech Institute,11Phoniatrics Unit, Otorhinolaryngology Department, Faculty of Medicine/Mansoura University,12PhoniatricsUnit,OtorhinolaryngologyDepartment,FacultyofMedicine/Beni- Suef University, 13Phoniatrics Unit, Otorhinolaryngology Department, Faculty o f Medicine/ Sohag University, 14Phoniatrics Unit, Otorhinolaryngology Department, Faculty of Medicine/Al-Azhar University, 15Psychiatry Department, Faculty of Medicine/ Cairo University
Sincere thanks extend to the secretaries: Samar Hussein and Eman Ragab, as well as the editor: Mohamed Salah
- Abbreviations
ADHD Attention deficit hyperactivity disorder
ARST Arabic Reading Screening Test
ASD Autism Spectrum Disorders
CLD Cultural modification
DLD Delayed Language Development
ELL English language learning
IQ Intelligence Quotient
L1 learner First language learner
L2 Learner Second language learner
LD Learning Disability
MADST Modified Arabic Dyslexia Screening Test
PA Phonologic awareness test
PTSD Post-traumatic stress disorder
RAN Rapid automatized naming
SMARTS Specific, Measurable, Applicable, Realistic, Timely, and Supported by research.
SLD Specific Learning Disability
WFD Word finding difficulty- Executive Summary
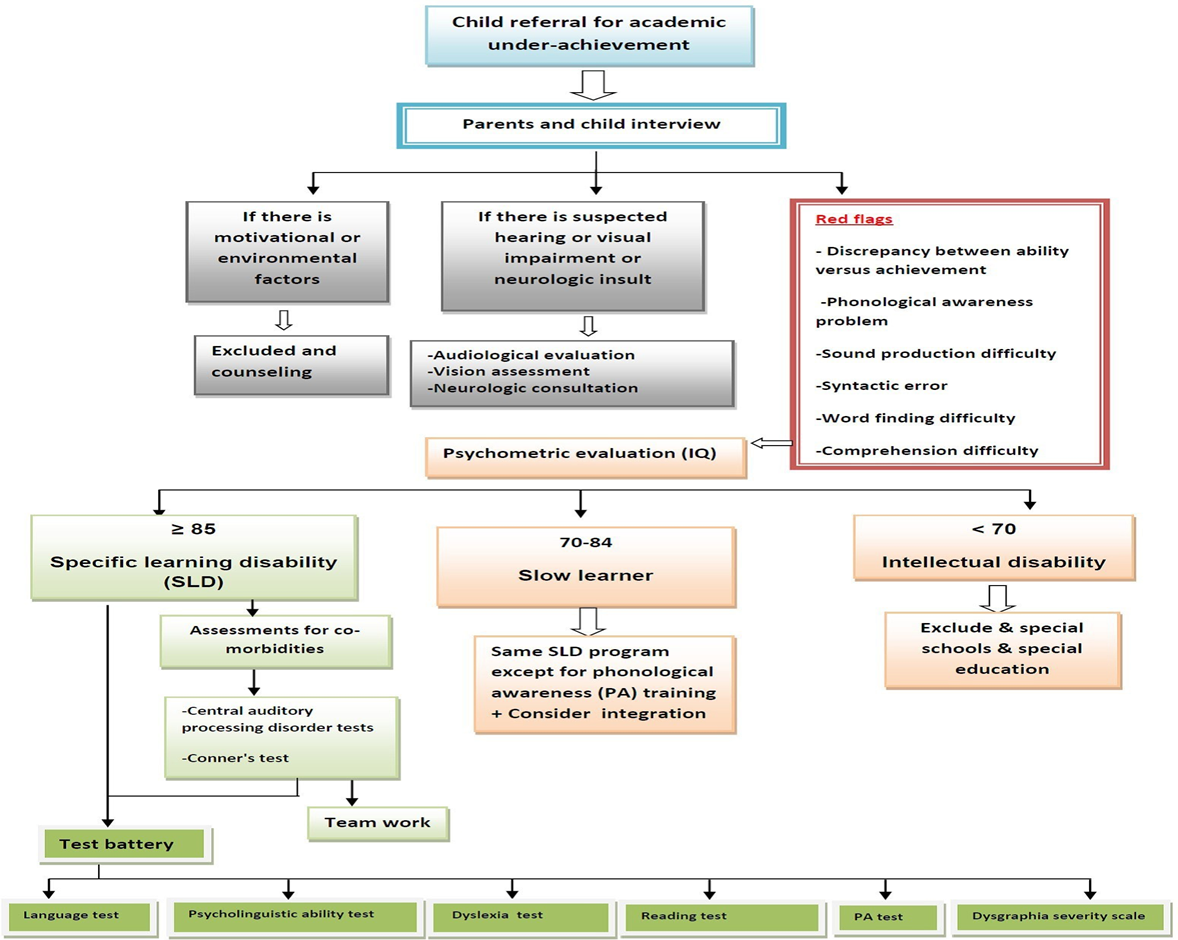
Common red flags for learning disabilities: • Discrepancy between child's ability versus his/her academic achievement. • Phonological awareness problem. • Sound production difficulty. • Syntactic errors. • Word finding difficulty. • Reading comprehension problems(Strong recommendation).
First step in assessment is to exclude other factors that might account for academic underachievement, such as: • Hearing impairment • Visual impairment (uncorrected errors) • Intellectual disabilities • Neurodevelopmental disorders • Environmental factors (e.g. inappropriate educational instruction) • Insufficient motivation (Strong recommendation).
Through psychometric evaluation (IQ assessment), the child is put in one of the following 3 categories: A. Specific learning disability (SLD) (if IQ≥ 85). These children will be subjected to SLD training program. B. Slow learner (if IQ 70-84). These children are candidates for "integration" and should receive same SLD training program except for phonological awareness training. C. Intellectual disability (if IQ < 70). These children need special schools and special education(Strong recommendation).
When the diagnosis of SLD is established, the following assessments should be undertaken: • Assessment of comorbidities: including central auditory processing disorders (CAPD) through special tests, and attention deficit hyperactivity disorder (ADHD) through Conner's test. • Assessments to delineate the areas of deficit, such as: Language test, psycholinguistic abilities test, dyslexia test, reading test, phonological awareness (PA) test, dysgraphia disability scale (Strong recommendation).
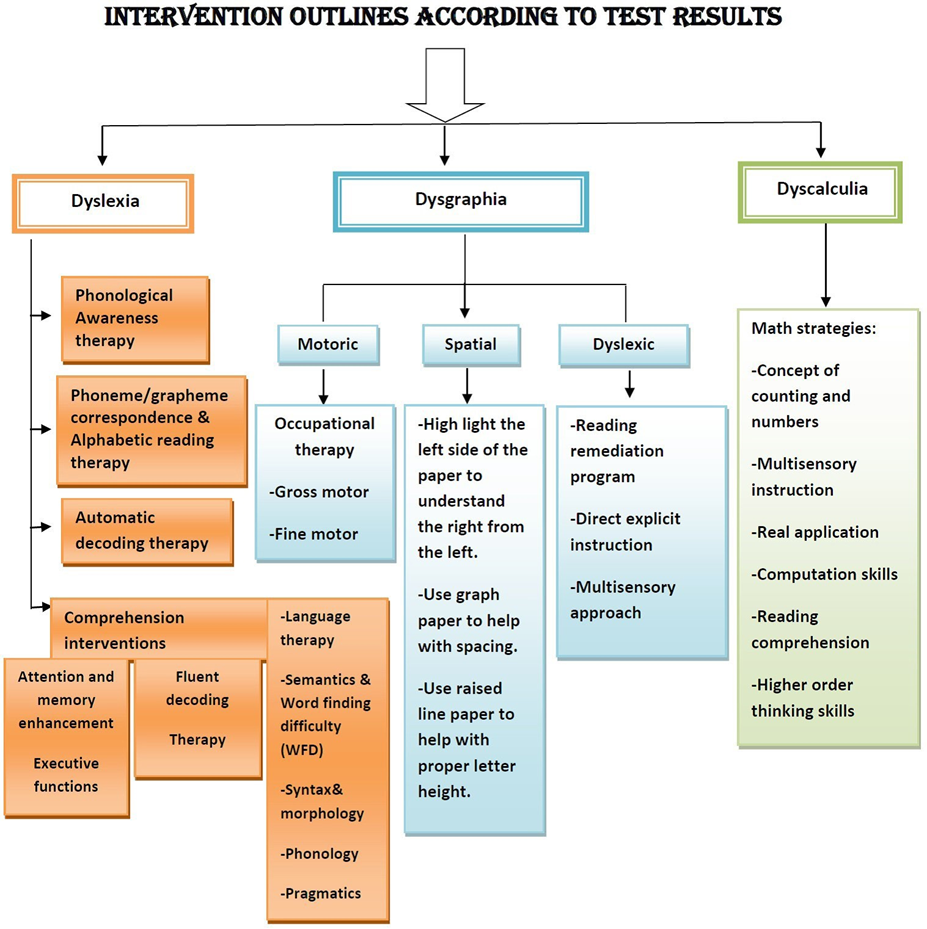
Management of SLD depends on its type as follows: a) Management of dyslexia includes: • Phonological awareness training. • Phoneme/grapheme correspondence & alphabetic reading therapy. • Automatic decoding therapy. • Interventions for reading comprehension. b) Management of dysgraphia is based on its type whether dyslexic, motoric, or spatial dysgraphia. Management of dyscalculia through specific mathematics strategies (Strong recommendation).
- Introduction, purpose, scope and audience
➡️Introduction
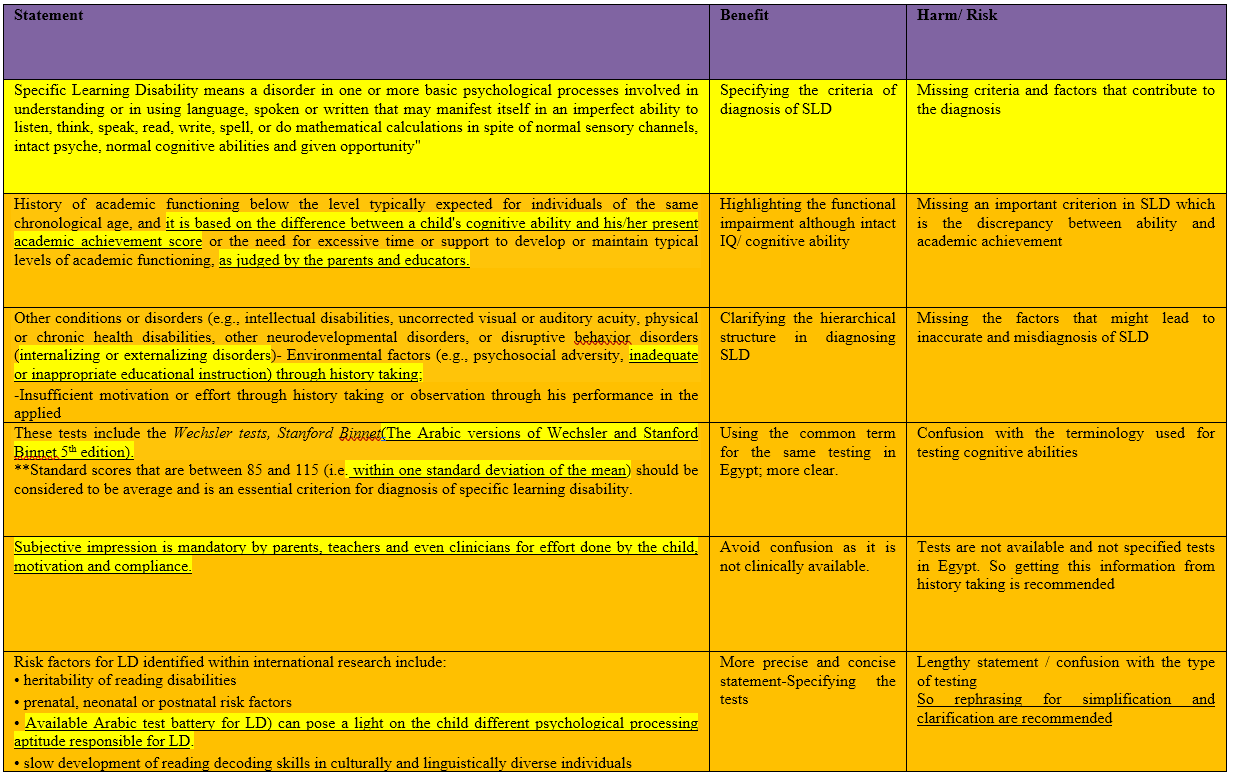
Specific Learning Disability(SLD)means a disorder in one or more basic psychological processes involved in understanding Or in using language ;spoken or written; that may manifest itself in an imperfectability to listen, think, speak ,read, write, spell or do mathematical calculations inspite of normal sensory channels, intact psyche, normal cognitive abilities and given opportunity.
➡️Scope: The scope of the guideline is to provide a brief overview of the current policy and practice of SLD diagnosis and rehabilitation. It will help guide when to consider SLD in school children and the different modifications and accommodations that will assist them at school.
➡️Target audience: Phoniatricians and speech and language therapists.
- Methods
➡️Methods of development
Stakeholder Involvement: Individuals who were involved in the development process. Included the above-mentioned Phoniatrics Chief Manager, Phoniatrics Executive Manager, Assembly Board, Grading Board and Reviewing Board.
Information about target population experiences was not applicable for this topic.
The adaptation cycle passed over: set-up phase, adaptation phase (Search and screen, assessment: currency, content, quality&/decision/selection) and finalization phase that included revision and external reviewing.
➡️Search Method
Pubmed, Medline, Egyptian knowledge Bank, Google Scholar
➡️Keywords
Specific learning disability, dyslexia, dyscalculia, ADHD
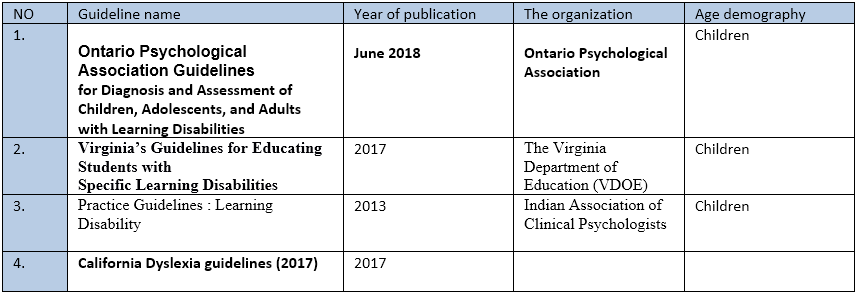
➡️Time period searched: From January 2013 to June 2018.
➡️Results
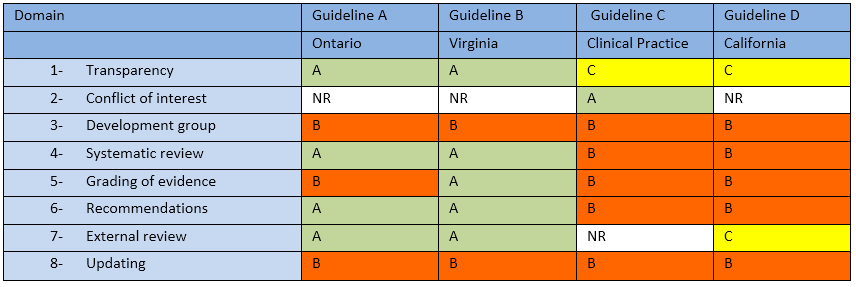
Fourguidelineswereassessedby4expertphoniatricians and the Ontario Psychological Association Guidelines for Diagnosis and Assessment of Children, Adolescents, and Adults with Learning Disabilities (June2018) (1) and Virginia’s Guidelines for Educating Students with Specific Learning Disabilities (2017) (2) had the highest scores as regards to the currency ,contents and quality .It was graded GRADE by11expertphoniatricians andreviewedby3expert reviewers to improve quality, gather feedback on draft recommendations.
The external review was done through a rating scale as well as open-ended questions.
➡️Setting: Primary, secondary and tertiary care centers & hospitals, and related specialties.
Interpretation of strong and conditional recommendations for an intervention
|
Audience |
Strong recommendation |
Conditional recommendation |
|
Patients |
Most individuals in this situation would want the recommended course of action; only a small proportion would not. Formal decision aides are not likely to be needed to help individuals make decisions consistent with their values and preferences. |
Most individuals in this situation would want the suggested course of action, but many would not |
|
Clinicians |
Most individuals should receive the intervention. Adherence to the recommendation could be used as a quality criterion or performance indicator. |
Different choices will be appropriate for individual patients, who will require assistance in arriving at a management decision consistent with his or her values and preferences. Decision aides may be useful in helping individuals make decisions consistent with their values and preferences. |
|
Policymakers |
The recommendation can be adopted as policy in most situations. |
Policy-making will require substantial debate and involvement of various stakeholders. |
WHO handbook for guideline development – 2nd ed.
Chapter 10, page 129
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to Decision frameworks (GRADE Working Group 2013)
|
Grade |
Definition |
|
High
|
We are very confident that the true effect lies close to that of the estimate of the effect. |
|
Moderate
|
We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different |
|
Low
|
Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. |
|
Very Low
|
We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect |
- Recommendations
The following statements and flowchart were adapted from the Guidelines from (Ontario & Virginia guidelines) which received the highest scores as regards the currency, contents, and quality.
Recommendations statements

Learning Disability Guideline Statements Guided by Ontario Guidelines
|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
References |
|
1.Criteriafor a Diagnosis of Learning Disability |
Specific Learning Disability means a disorder in one or more basic psychological processes involved in understanding or in using language, spoken or written that may manifest itself nan imperfect ability to listen ,think, speak, read, write, spell, or do mathematical calculations in spite of normal sensory channels, intact psyche, normal cognitive abilities and given opportunity”. |
Very Low |
Conditional |
Expert opinion
(Review article) |
3 |
|
2.Historyof academic impairment |
History of academic functioning below the level typically expected for individuals of the same chronological age, and it is based on the difference between a child’s cognitive ability and his/her present academic achievement score or the need for excessive time or support to develop or maintain typical levels of academic functioning, as judged by the parents and educators. |
Moderate
|
Strong |
Systematic review |
4 |
|
3.Evidencethatthe difficulties in reading, writing ,or
mathematics cannot be accounted for primarily by other factors |
Other conditions or disorders(e.g., intellectual disabilities, uncorrected visual or auditory acuity, physical or chronic health disabilities, other neurodevelopmental disorders, or disruptive behavior disorders (internalizing or externalizing disorders)- Environmental factors(e.g. Psychosocial adversity, inadequate or inappropriate educational instruction) through history taking: -Insufficient motivation or effort through history taking or observation through his performance in the applied tests; -Cultural or linguistic diversity through history taking. |
Low |
Strong |
Case-Control study |
5 |



|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
References |
|||
|
4.Assess abilities essential for thinking and reasoning. |
These tests include the Wechsler tests, Stanford Binnet (The Arabic versions of WechslerandStanfordBinnet5thedition). **Standard scoresthatarebetween85 and115 (i.e. Within one standard deviation of the mean) should be considered to be average and is an essential criterion for diagnosis of specific learning disability. |
Moderate |
Strong |
Systematic review |
6
|
|||
|
5.Assess and rule out other factors that could better explain the pattern of results, including Effort ,motivation and non-compliance with instructions
|
Subjective impression is mandatory by parents, teachers and even clinicians for effort done by the child, motivation and compliance. |
Low |
Strong |
Observational study |
7 |
|||
|
6.Evidence of risk factors for LD and other learning difficulties
|
Risk factors for LD identified within International research include: •heritability of reading disabilities •prenatal ,Newborn or postnatal risk factors •Available Arabic test battery for LD) can pose a light on the child different psychological processing aptitude responsible for LD. |
Moderate |
Strong
|
Systematic review |
8
9
|
|||
|
|
•slow development of reading decoding Skills in culturally and linguistically diverse individuals. |
|
|
|||||
|
7.Assess academic achievement |
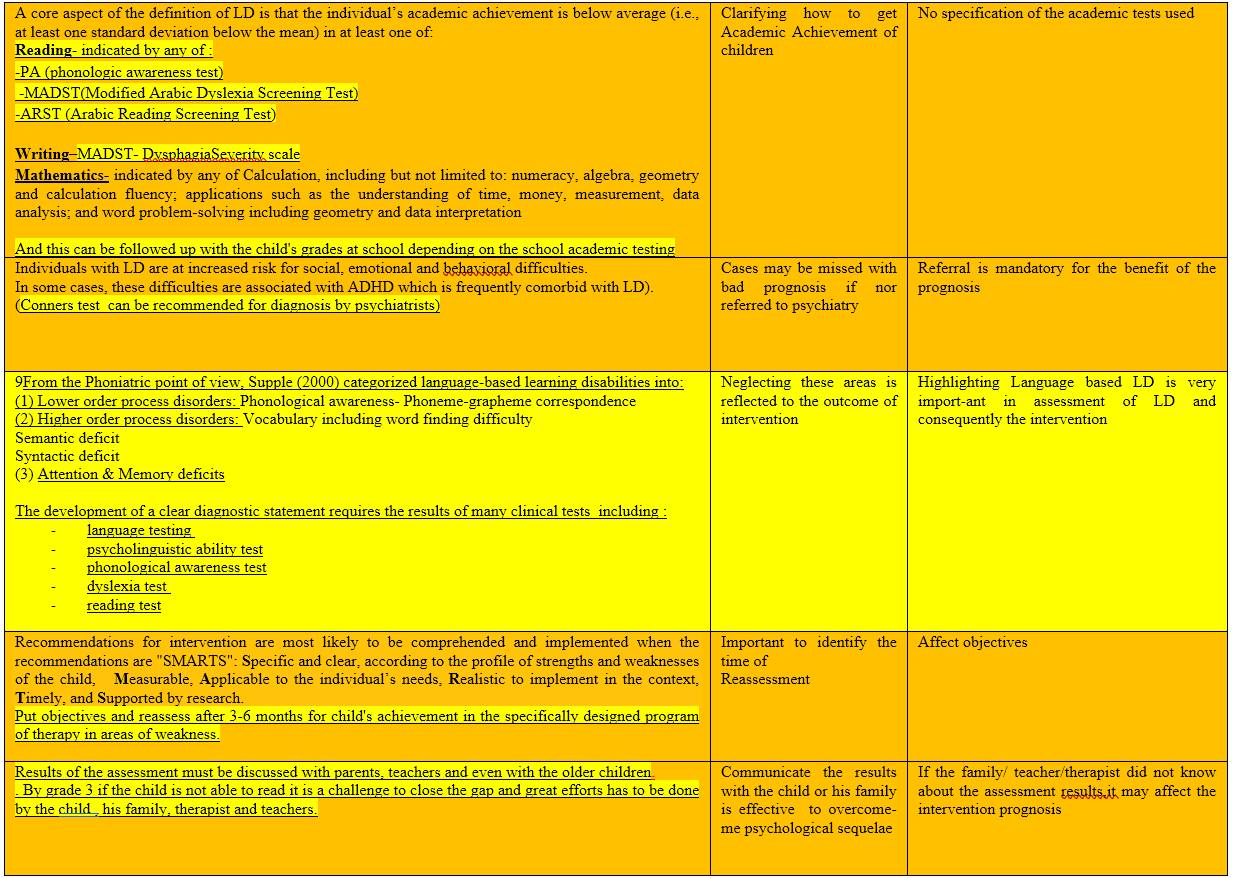
A core aspect of the definition of LD is that the individual’s academic achievement is below average(i.e.,at least one standard deviation below the mean)in at least one of: Reading- indicated by any of : -PA(phonologic awareness test) -MADST(Modified Arabic Dyslexia Screening Test) -ARST(Arabic Reading Screening Test) Writing–MADST-Dysphagia Severity scale Mathematics- indicated by any of Calculation, including but not limited to: numeracy, algebra, geometry and calculation fluency; applications such as the understanding of time, money, measurement, data analysis; and word problem-solving including geometry and data interpretation. |
Very Low |
Strong |
Expert opinion
|
||||
|
|
And this can be followed up with the child’s grades at school depending on the school academic testing. |
|
|
|||||




|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
References |
|
8.Assesscomorbid emotional and behavioral problems documented by clinical judgment and testing |
-Individuals with LD are at increased risk for social, emotional and behavioral difficulties. In some cases, these difficulties are associated with ADHD which is frequently comorbid with LD). (Conner’s test can be recommended to aid diagnosis) |
Low
|
Strong
|
Observational Study (Cohort) |
10 |
|
9.Developa formulation and diagnostic statement in accordance with the above criteria for a diagnosis of LD |
From the Phoniatric point of view, Supple (2000) categorized language-based learning disabilities into: (1) Lower order process disorders: Phonological awareness-Phoneme- grapheme correspondence (2)Higher order process disorders: Vocabulary including word finding difficulty Semantic deficit Syntactic deficit (3) Attention & Memory deficits The development of a clear diagnostic statement requires the results of many clinical tests including: Language testing • Psycholinguistic ability test • Psychical awareness test • Dyslexia test • Reading test • Dysgraphia Severity scale. |
Low |
Strong |
Cohort observational study |
11 |


|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
References |
||
|
10.Identify the types of evidence-based and realistic supports and interventions that are required |
Recommendations for intervention are most likely to be comprehended and implemented when there commendations are “SMARTS”: Specific and clear, according to the profile of strengths and weaknesses of the child, Measurable, Applicable to the individual’s needs, Realistic to implement in the context, Timely, and Supported by research. |
Very Low |
Strong |
Expert opinion |
12
|
||
|
|
Put objectives and reassess after 3-6 Months for child’s achievement in the specifically designed program of therapy in areas of weakness. |
|
|||||
|
11.Communicate the results of the assessment, the diagnosis and recommendations |
Results of the assessment must be discussed with parents, teachers and even with the older children. By grade 3 if the child is not able to read it is a challenge to close the gap and great efforts has to be done by the child, his family, therapist and teachers. |
Very Low |
Strong |
Expert Opinion (Review article) |
13
|
||
|
12.Theoptimalageto firstscreens for and diagnoses LD? |
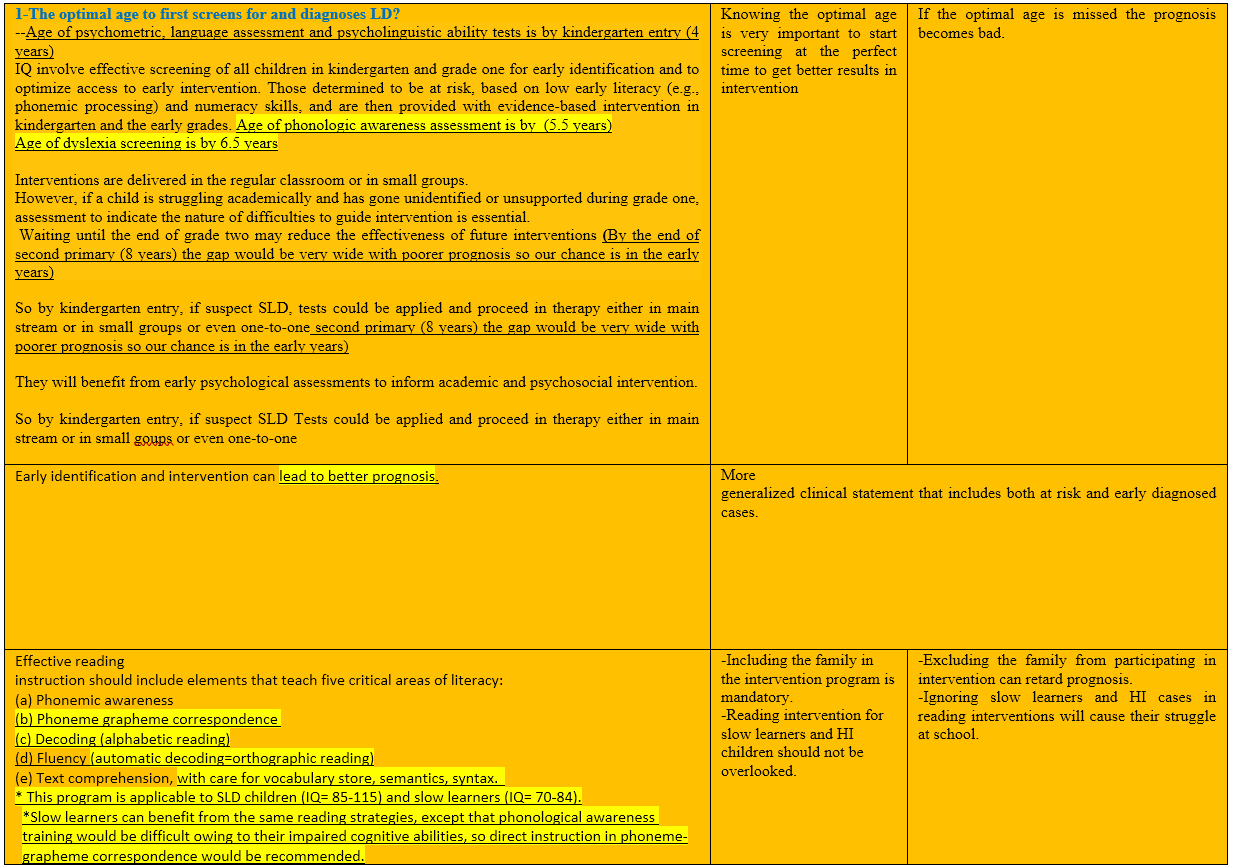
-Age of psychometric, language assessment and psycholinguistic ability tests is by kindergarten entry (4 years). IQ involve effective screening of all children in kindergarten and grade one for early identification and to optimize access to early intervention. Those determined to be at risk, based on low early literacy (e.g., phonemic processing)and numeracy skills, and are then provided with evidence-based intervention in kindergarten and the early grades. Age of phonologic awareness assessment is by (5.5years). Ageofdyslexiascreeningisby6.5 years. Interventions are delivered in the regular classroom or in small groups. However, if a child is struggling academically and has gone unidentified or unsupported during grade one, assessment to indicate the nature of difficulties to guide intervention is essential. Waiting until the end of grade two may reduce the effectiveness of future interventions (By the end of second primary (8years) the gap would be very wide with poorer prognosis so our chance is in the early years). So by kindergarten entry, if suspect SLD, tests could be applied and proceed in therapy either in main stream or in small groups or even one-to-one. |
moderate |
Strong |
Systematic review |
14 |
||



|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
References |
|
13.Childrenat disproportionate risk for learning challenges |
Such as children with early symptoms or diagnosis of - ADHD. -DLD, ASD. -Children with complex medical conditions: (e.g. extreme prematurity, congenital heart disease). -Early brain injury (e.g .Newborn stroke, brain tumor, traumatic brain injury). - Epilepsy. Children with learning co-morbidities will also benefit from early assessment with a focus on contributing to school-based support. |
Very Low |
Strong |
Review article (Expert opinion) |
15 |
|
14- Whatadaptations are required for assessments of Culturally and Linguistically Diverse (CLD) individuals experiencing learning difficulties as regard language and literacy skills |
For the First (L1) and Second (L2) learners • Consider a diagnosis of LD in L2 individuals who have hardwood more years of English or French reading instruction and have below average word-level reading and spelling skills. •Examine the types of errors that individuals make on language Consider positive transfer(e.g., they may use words that are similar intheirL1to understandtheL2),and negative transfer (they may apply grammatical structures that are correct in theirL1 totheirL2 when that is not appropriate). •Compare the functioning of the individual with siblings from the same context. •Assess in the individual’s first language When appropriate. •Assess cognitive processes(phonological processing, rapid automatized naming “RAN”, and non-word repetition). •Consider that If phonological processing scores are below average that this may represent a Learning Disability, rather than being due to English language learning “ELL” status alone. •Supplement standardized cognitive and achievement tests including nonverbal test with few instructions and use clinical judgment when interpreting test scores. |
Low |
Strong |
Cohort study
|
16
|


|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
References |
|
15.Social,Emotional and Behavioral Assessment in CLD Individuals |
•The following strategies are recommended to decrease cultural and linguistic loading for CLD. • Use multiple sources (self- family and teacher reports)and methods (observations, interviewing, formal objective rating scales, and informal projective tests such as drawings and sentence completions). •Use standardized rating scales written in the individual’s or parent’sL1. -Consider acculturation effects(i.e. Effects of cultural modification of CLD individuals caused by merging of cultures). •Analyze narratives provided by the individual and family members. -Be sensitive to signs of post-traumatic stress disorder “PTSD”, and other disorders that are associated with loneliness, trauma, and immigration struggles. |
Very Low |
Strong |
Book chapter
(Expert opinion) |
17 |
|
16.Issuesshould be considered when diagnosing LD in individuals with very superior intellectual ability |
Above average intelligence does not negate the possibility of having areas of strengths and weaknesses in major areas of academic functioning and psychological processing. Maddocks (2018) found that children with high IQ could be diagnosed as LD when taking into consideration both intra- individual ability- achievement discrepancy criteria and academic impairment. |
Moderate |
Strong |
Systematic review |
18
|


Learning Disability Guidelines Statements Guided by Virginia Guidelines
|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study stype |
references |
|
Early identification |
Early identification and intervention can lead to better prognosis. |
Moderate |
Strong |
Systematic review Systematic review
|
19
20 |
|
Reading strategies |
Effective reading instruction should include elements that teach five critical areas of literacy: (a)Phonemic awareness. (b)Phoneme grapheme correspondence. (c) Decoding (Alphabetic reading). (d) Fluency (Automatic decoding=orthographic reading). (e)Text comprehension, with care for vocabulary store, semantics, syntax. *This program is applicable to SLD children(IQ= 85-115) and slow learners (IQ= 70-84). *Slow learners can benefit from the same reading strategies ,except that phonological awareness training would be difficult owing to their impaired cognitive abilities, codirect instruction in phoneme-grapheme correspondence would be recommended.=3.6. |
moderate
moderate |
Strong
strong |
Systematic review
Systematic review
|
21
22 |
|
Reading fluency striges |
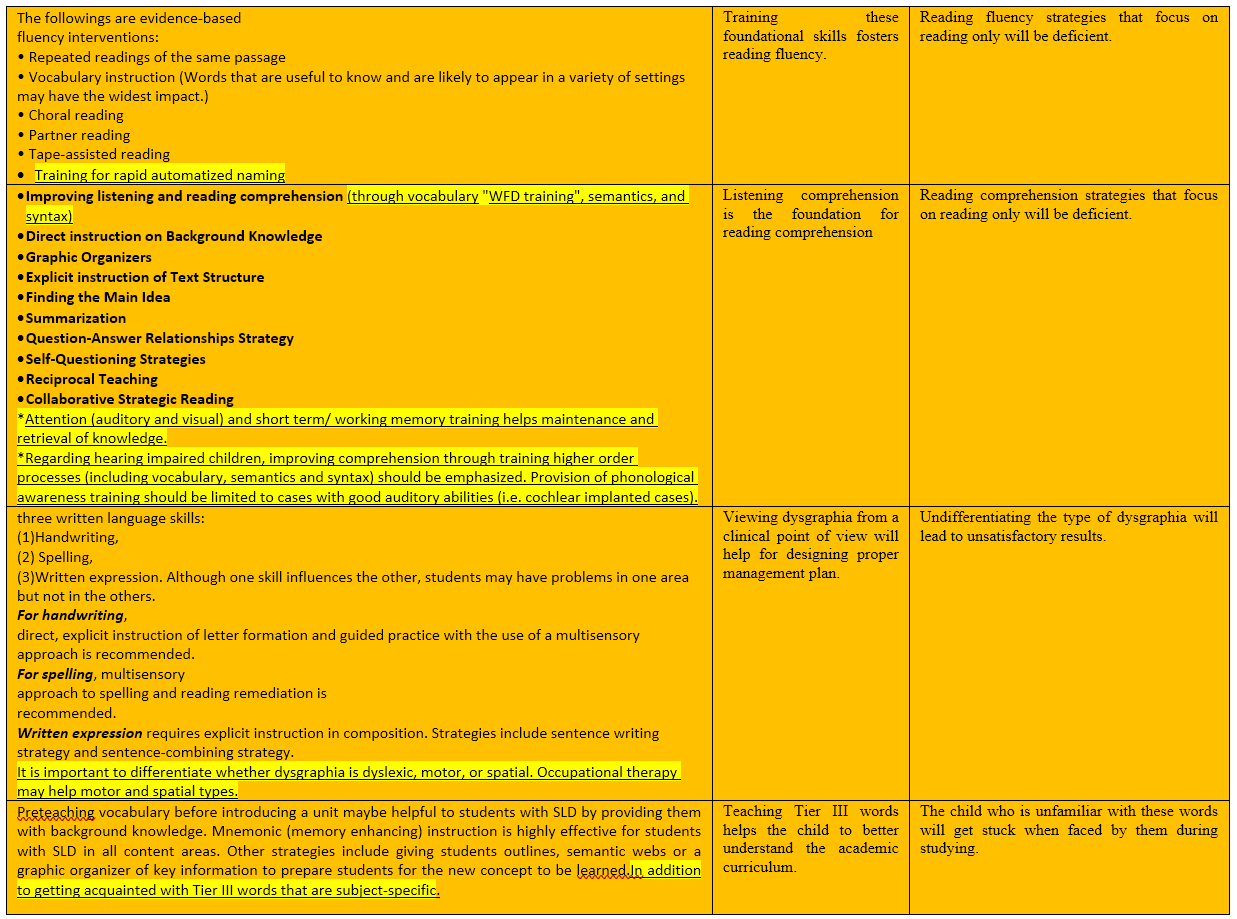
The followings are evidence-based fluency interventions: • Repeated readings of the same passage. • Vocabulary instruction (Words that are useful to know and are likely to appear in variety of settings may have the widest impact.). • Choral reading. • Partner reading. • Tape-assisted reading. • Training for rapid automatized naming. |
Very Low |
Strong |
Expert opinion
(Review article)) |
23 |



|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
reference |
|
Reading Comprehension-on strategies |
• Improving listening and reading comprehension (through vocabulary “WFD tuning”, semantics, and syntax). • Direct instruction on Background Knowledge. • Graphic Organizers. • Explicit instruction of Text Structure. • Finding the Main Idea. • Summarization. • Question-Answer Relationships Strategy. • Self-Questioning Strategies. • Reciprocal Teaching. • Collaborative Strategic Reading. *Attention (auditory and visual) and short term/ working memory training helps maintenance and retrieval of knowledge. *Regarding hearing impaired children, improving comprehension through training higher order processes (including vocabulary, semantics and syntax) should be emphasized. Provision of phonological awareness training should be limited to cases with good auditory abilities (i.e. cochlear implanted cases). |
Very low
moderate
moderate |
Strong
strong
Strong |
Expert opinion
(Review article)
Systematic review
Research based practice |
24
25
26
|
|
Written language strategies |
Three written language skills: (1) Handwriting. (2)Spelling. (3)Written expression .Although one skill influences the other, students may have problems in one area but not in the others. For handwriting direct, explicit instruction of letter formation and guided practice with the use of a multisensory approach is recommended. For spelling, multisensory approach (using visual, auditory, tactile, and kinesthetic modalities) and reading remediation is recommended. Written expression through sentence writing strategy and sentence-combining strategy. It is important to differentiate whether dysgraphia is dyslexic, motor, or spatial. Occupational therapy may help motor and spatial types. |
moderate
Very Low |
Strong
Strong |
Systematic review
Expert opinion
(Review article) |
27
28 |
|
Mathematics strategies |
Explicit instruction should be provide during manipulative, cognitive strategies ,using visual representations while solving mathematical problems, using graphic organizers to solve systems of linear equations, etc. |
Moderate |
Strong |
systematic review |
29 30
|



|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
reference |
|
|
Social studies and science strategies
|
Effective strategies include: -Pre teaching vocabulary before introducing a unit. -Mnemonic (memory enhancing) instruction. -Giving students outlines, semantic webs or a graphic organizer of key information. -Getting acquainted with Tier III words(which are Low-frequency, subject-specific words). |
|
Strong |
Systematic review |
31 |
|
|
Accommodations
|
Accommodations are consideredtobe “changes to the delivery of instruction, method of student performance, or method of assessment that do not significantly change the content or conceptual difficulty level of the curriculum”. Examples of accommodations Include: a) Use of mnemonics strategy. b)Cooperative learning groups. c) Modeling procedures. d)Word processors. e) Providing preferential seating. f)Providing special lighting or acoustics. g)Oralversus written response. h)Administering a test in several timed sessions. i) Use of assistive technology. |
|
Strong |
Systematic review |
32
|
|
|
Modifications
|
Modifications are changes to the curricular content, changes to the conceptual difficulty level of the curriculum, or changes to the objectives and methodology. These involve more significant changes than accommodations. |
moderate |
Strong |
Systematic review |
32 |
|
|
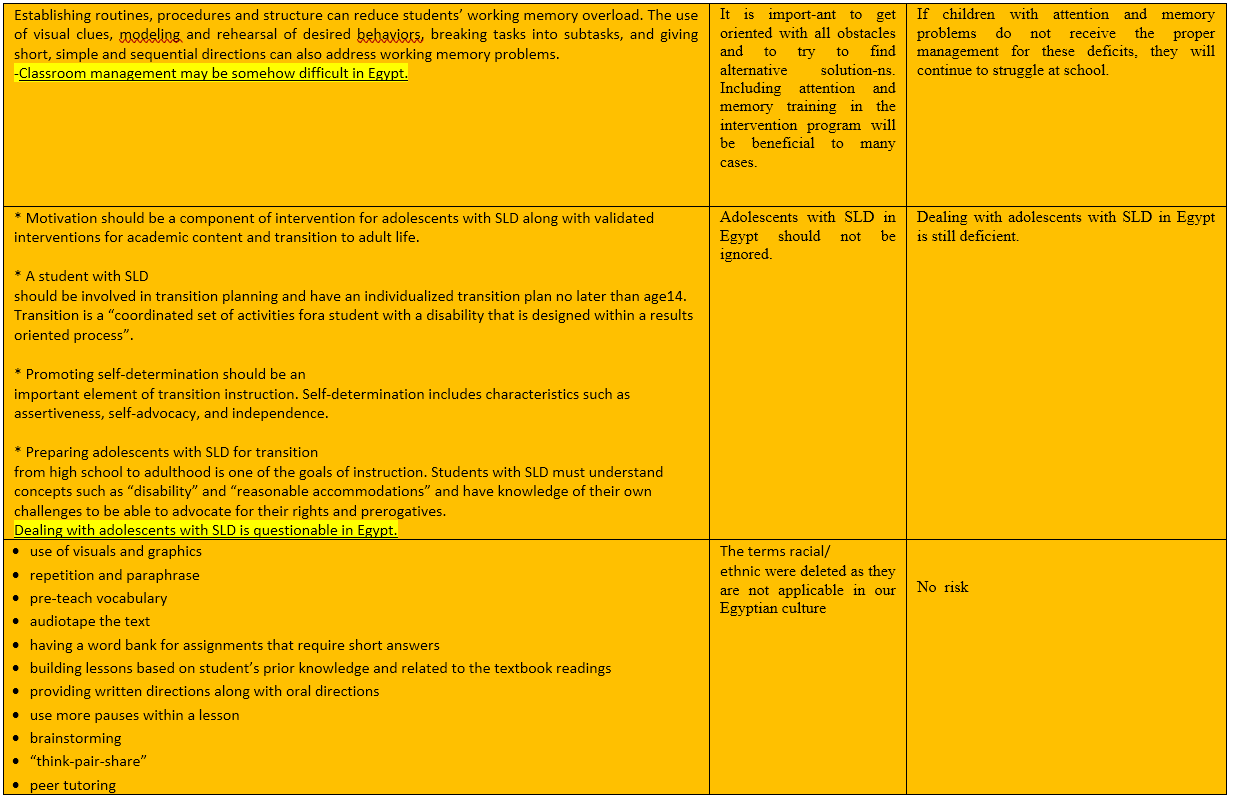
Classroom management
|
Establishing routines can reduce students ‘working memory overload. The use of visual clues, modeling and rehearsal of desired behaviors, breaking tasks into subtasks can also address working memory problems. Classroom management may be somehow difficult in Egypt. |
Moderate |
Strong |
Systematic review |
33 |
|




|
Clinical questions |
Action recommendation |
Evidence Quality |
Strength of Recommendation |
Study type |
reference |
|
Adolescents with SLD |
*Motivation * A student with SLD should be involved in transition planning and have an individualized transition plan no later than age 14. *Promoting self-determination which includes characteristics such as assertiveness, self- advocacy, and independence. * Preparing adolescents with SLD for transition from high school to adulthood is one of the goals of instruction, to enable them to advocate for their rights and prerogatives. Dealing with adolescents with SLD is questionable in Egypt. |
moderate
moderate |
strong
Strong |
Systematic review
Systematic review |
34
35 |
|
Students from diverse backgrounds with SLD |
Use of visuals and graphics, repetition and paraphrase, pre-teach vocabulary, audiotape the text, having a word bank for assignments that require short answers. Providing written directions along with oral directions, use more pauses within a lesson. Brainstorming, “think-pair-share”, peer tutoring. |
Moderate
moderate |
strong
Strong |
Systematic review
Systematic review |
36
37 |
|
The Twice- Exceptional Students
|
*Twice-exceptional students are those learners who meet criteria for being identified as both gifted and having a specific learning disability. * Teachers must consider the students ‘strengths (e.g., problem solving, metacognition)and problem areas(e.g., basic skills, organization). Twice-exceptional students need teachers who will provide them with emotional support, effective instruction, accommodations. (e.g., calculators, spell-checkers),and skills for self-advocacy. |
moderate
moderate
|
Strong
strong |
Systematic review Systematic review |
38
39 |



- Research needs
The following studies are needed to be conducted;
1- Remediation program of LD on high risk group like preschoolers Egyptian SLI children
2- Applying protocol of assessment of learning disability in bilingual children with academic difficulty.
3- Determination of most accurate & sensitive psychometric tests (Stanford vs. Wechsler) in assessment of LD by correlation study between findings of psychometric tests with Learning disability assessment testing.
4- Standardization of PA tests in preschool and school aged Egyptian children.
5- Applying assessment protocol of LD on at high risk group children with ADHD, SLI to determine the severity and profile/ type of their learning difficulty.
6- Home based rehabilitation program of memory training in children with learning disability.
7- Central auditory processing in children with learning disability
8- Pragmatic testing of children with learning disability.
- Monitoring and evaluating the impact of the guideline
Monitoring/ Auditing Criteria: to assess guideline implementation or adherence to recommendations. This is accomplished if the child begins to get benefit from the used appropriate strategies addressing his difficulties and when the needed recommended classroom management assisted his academic performance.
Clinicians should be able to:
· Acquire the a full developmental history and the academic history of the child from the parents
· Exclude other causes of low academic underachievement as low intellectual ability, impaired sensory functions, etc.
· Is the child’s recent IQ test in the average range?
· Has the child other comorbid emotional or behavioral comorbidities?
· Provide effective strategies for reading, fluency, reading comprehension to address the difficulties in these areas
· Provide advice for classroom management as establishing routines can reduce students ‘working memory overload. The use of visual clues, modeling and rehearsal of desired behaviors, breaking tasks into subtasks can also address working memory problems.
All clinicians should be aware and informed to consider the following red flags:
· Discrepancy between ability versus achievement
· Phonological awareness problems
· Sound production difficulty
· Syntactic error
· Word finding difficulty
· Comprehension difficulty
In order to monitor the efficacy of the rehabilitation program: The following tests can be used:
· iQ test
· Arabic Language test
· Phonological awareness test
· Modified Arabic dyslexia screening test
· Arabic reading screening test
· Dysgraphia severity scale
- Updating of the guideline
Updating Procedure:
Any recommendation of this guideline will be updated when new evidence that could potentially impact the current evidence base for this recommendation is identified. If no new reports or information are identified for a particular recommendation, the recommendation will be revalidated. The focus will be on recommendations supported by very-low- or low certainty evidence and where new recommendations or a change in the published recommendations may be needed.
- References
1.BealL,etal.ConsensusStatementonDiagnosisand Assessment of Children, Adolescents, and Adults with Learning Disabilities. Ontario Psychological Association.2018.
2.WatsonS,etal.Virginia’sGuidelinesforEducating StudentswithSpecific LearningDisabilities.Virginia Departmentof Education Division of Special EducationandStudent Services. 2017.
3. Roitsch, Jane & Watson, Silvana. (2019). An Overview of Dyslexia: Definition, Characteristics, Assessment, Identification, and Intervention. Science Journal of Education. 7. 81. 10.11648/j.sjedu.20190704.11.
4.Kovachy, Vanessa & Adams, Jenna & Tamaresis, John & Feldman, Heidi. (2014). Reading abilities in school-aged preterm children: A review and meta-analysis. Developmental Medicine & Child Neurology. 57. 10.1111/dmcn.12652.
5. Ozernov-Palchik O, Centanni TM, Beach SD, May S, Hogan T, Gabrieli J. Distinct neural substrates of individual differences in components of reading comprehension in adults with or without dyslexia. Neuroimaging. 2021 Feb 1;226:117570. doi: 10.1016/j.neuroimage.2020.117570. Epub 2020 Nov 19. PMID: 33221445; PMCID: PMC7855566.
6. DeRight, J., & Carone, D. A. (2013). Assessment of effort in children: A systematic review. Child Neuropsychology, 21(1), 1-24.
7.Kirkwood, M. W., & Kirk, J. W. (2010). The base rate of suboptimal effort in a pediatric mild TBI sample: Performance on the Medical Symptom Validity Test. Clinical Neuropsychologist, 24, 860 – 872
8-Huang J, Zhu T, Qu Y, Mu D. Prenatal, Perinatal and Neonatal Risk Factors for Intellectual Disability: A Systemic Review and Meta-Analysis. PLoS One. 2016 Apr 25;11(4):e0153655. doi: 10.1371/journal.pone.0153655. PMID: 27110944; PMCID: PMC4844149.
9.Geva, E., & Wiener, J. (2015). Psychological assessment of culturally and linguistically diverse children and adolescents: A practitioner’s guide. New York, NY: Springer
10. Milligan, K., Phillips, M., & Morgan, A. (2015). Tailoring social competence interventions for children with learning disabilities. Journal of Child and Family Studies, 25, 856-869
11.Rapcsak SZ, Beeson PM, Henry ML, Leyden A, Kim E, Rising K, Andersen S, Cho H. Phonological dyslexia and dysgraphia: cognitive mechanisms and neural substrates. Cortex. 2009 May;45(5):575-91. doi: 10.1016/j.cortex.2008.04.006. Epub 2008 Jun 5. PMID: 18625494; PMCID: PMC2689874.
12.Ontario Ministry of Education (2013). Policy/program memorandum No. 156: Supporting transitions for students with special education needs. Retrieved from http://www.edu.gov.on.ca/extra/eng/ppm/ppm156.pdf
13.Wiener, J., & Costaris, L. (2012). Teaching psychological report writing: Content and process. Canadian Journal of School Psychology, 29(2), 119-135
14. Baron, I. S., & Anderson, P. A. (2012). Neuropsychological Assessment of Preschoolers. Neuropsychology Review, 22, 311–312
15.Sahoo MK, Biswas H, Padhy SK. Psychological Co-morbidity in Children with Specific Learning Disorders. J Family Med Prim Care. 2015 Jan-Mar;4(1):2015. doi: 10.4103/2249-4863.152243. PMID: 25810984; PMCID: PMC4367000
16. Cormier, D. C., Wang, K., & Kennedy, K. E. (2016). Linguistic demands of the oral directions for administering the WISC-IV and WISC-V. Canadian Journal of School Psychology, 31(4), 1-15.
17.Barkley, R. A. (2015) Comorbid Psychiatric Disorders and Psychological Maladjustment in Adults with ADHD. In R. A. Barkley (Ed.), Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (4th ed., pp. 343-355). New York, NY: Guilford Press.
18. García-Martínez I, Gutiérrez Cáceres R, Luque de la Rosa A, León SP. Analysing Educational Interventions with Gifted Students. Systematic Review. Children (Basel). 2021 May 3;8(5):365. doi: 10.3390/children8050365. PMID: 34063631; PMCID: PMC8147618.
19- O’Shaughnessy, T. E., Lane, K. L., Gresham, F. M., &Beebe-Frankenberger, M. E. (2003). Children placed at risk for learning and behavioral difficulties. Remedial and Special Education, 24, 27-35.
20- Steele, M. M. (2004). Making the case for early identification and intervention for young children at risk for learning disabilities. Early Childhood Education Journal, 32, 75-79.
21- Vaughn, S. & Linan-Thompson, S. (2003). What is special about special education for students with learning disabilities? Journal of Special Education, 37, 140-147.
22- Ritchey, K. D. (2011). The first “R”: Scientifically-based reading instruction for students with learning disabilities. Theory Into Practice, 50, 28-34.
23- Berninger, V. W., & Wolf, B. J. (2009). Teaching students with dyslexia and dysgraphia: Lessons from teaching and science.Baltimore, MD: Brookes Publishing Company
24- Caldwell, J. S., & Leslie, L. (2005). Intervention strategies tofollow reading inventory assessment: So what do I do now? Boston, MA: Pearson.
25- Dean, D., & Grierson, S. (2005). Re-envisioning readingand writing through combined text picture. Journalof Adolescent and Adult Literacy, 48, 456-488.
26- Trabasso, T., & Bouchard, E. (2002). Teaching readershow to comprehend text strategically. In C. C.Block & Presley (Eds.), Comprehension instruction: Research-based best practices (pp. 176-200). New York,NY: Guilford Press.
27- wanzek,J., Stevens, E. A; Williams, K.J. (2018). Current evidence on the effects of intensive early reading interventions. Journal of learning disabilities,51,612-624.
28- Saddler, B., & Asaro-Saddler, K. (2010). Writing better sentences: Sentence-combining instruction in the classroom. Preventing School Failure, 54, 159-163.
29-Geary, D. C. (2004). Mathematics and learning disabilities.Journal of Learning Disabilities, 37, 4-15. DOI:10.1177/00222194040370010201
30- Geary, D. C., Hoard, M. K., Nugent, L., & Bailey, D. H. (2012). Mathematical cognition deficits in children with learning disabilities and persistent low achievement: A five-year prospective study. Journal of Educational Psychology, 104(1), 206-223
31- Cohen, A. S., Gregg, N., & Deng, M. (2005). The role of extended time and item content on a high-stakes mathematics test. Learning Disabilities Research &Practice, 20, 225-233.
32- Gregg, N., & Nelson, J. M. (2012). Meta-analysis on the effectiveness of extra time as a test accommodation for transitioning adolescents with learning disabilities: More questions than answers. Journal of Learning Disabilities, 45, 128-133.
33- Watson, S. M. R., Gable, R. A., Gear, S. B., & Hughes, K.C. (2012). Scientifically-based strategies for improving the reading comprehension of secondary students :Implications for students with learning disabilities. where are we going? Gifted Child Quarterly, 55, 3-17.
34- Deshler, D. D. (2005). Adolescents with learning disabilities: Unique challenges and reasons for hope. Learning Disability Quarterly, 28, 122-124.
35- Lackaye, T., & Margalit, M., Ziv, O., & Ziman, T. (2006).Comparisons of self-efficacy, mood, effort, and hope between students with learning disabilities and theirnon-LD-matched peers. Learning Disabilities Research &Practice, 21, 111-121.
36- Lane, K. L., Carter, E. W., Pierson, M. R., & Glaeser, B. C.(2006). Academic, social, and behavioral characteristics of high school students with emotional disturbance or learning disabilities. Journal of Emotional and Behavioral Disorders, 14, 108-117.
37- Garcia, S. B., & Tyler, B-J. (2010). Meeting the needs of English language learners with learning disabilities in the general curriculum. Learning Disabilities Research & Practice, 49, 113-120.
38- Nicpon, M. F., Allmon, A., Sieck, B., & Stinson, R.D.(2011). Empirical investigation of twice exceptionality: Where have we been and where are we going? Gifted Child Quarterly, 55, 3-17.
39- Schultz, S. M. (2012). Twice-exceptional students enrolled in advanced placement classes. Gifted Child Quarterly,56,- Annexes
Editorial Independence:
· This guideline was developed without any external funding.
· All the guideline development group members have declared that they do not have any competing interests.
Annex1: Guideline Flowchart
Modifiedlearning disability flow chart for assessment
Annex2: Tables of appraisal of selected guidelines:Currency (table 1), Content (table 2) and Quality (table 3) of the selected guidelines.
1- Assessment of currency table:
2- Assessment of content table:
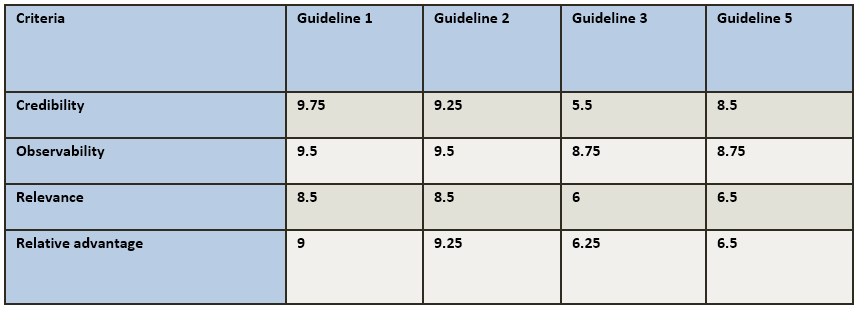
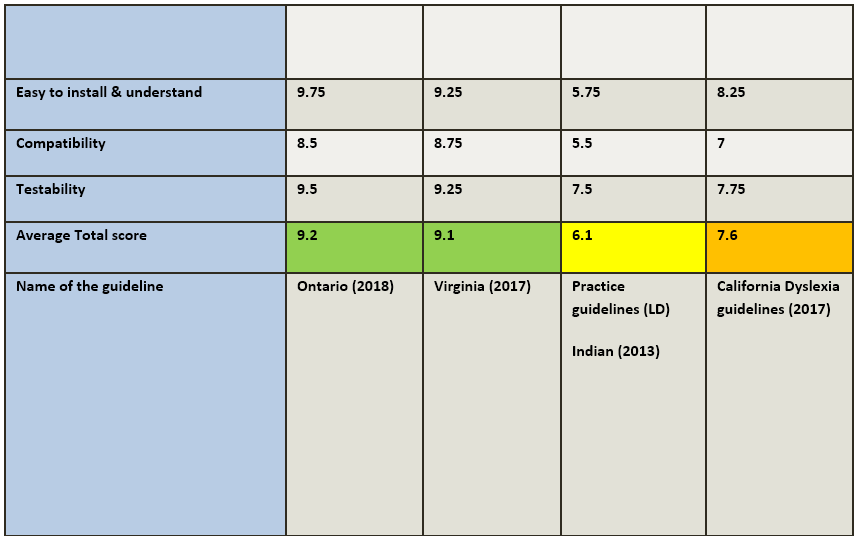
3- Assessment of quality (CPG Appraisal tool)
Annex 3: The risks and benefits of added and/or modified statements
(Modifications & Additional Statements)