First Part
| Site: | EHC | Egyptian Health Council |
| Course: | Procedural work guide for the burns unit |
| Book: | First Part |
| Printed by: | Guest user |
| Date: | Monday, 23 December 2024, 5:10 PM |
- Preparation
Central Nursing Administration
Dr. Kawthar Mahmoud Mahmoud Head of the Central Nursing Administration
Dr. Nevin Abd Rab Al-Nabi Muhammad, General Director of Therapeutic Nursing Department
Prof. Amany Farouk Mohamed, Senior Nursing Specialist at the Central Administration of Nursing
Prof. Azza Jalal Ahmed, Nursing specialist at the Central Administration of Nursing
Prof. Hanan Amin Shousha, Nursing specialist at the Central Administration of Nursing
Prof. Yasmine Sayed Abdel Basset, A nursing specialist in the Central Administration of Nursing
Prof. Marwa Mohamed Hassan, Nursing specialist at the Central Administration of Nursing
Prof. Ahmed Youssef Abdullah, Nursing specialist in the Central Administration of Nursing
A.T. Angham Hamdy Abdel Khaleq, Nursing specialist at the Central Administration of Nursing
Prof. Mohamed Abdel Ghani Youssef, Nursing specialist in the Central Administration of Nursing
Prof. Taha Mohamed Ahmed, Nursing specialist at the Central Administration of Nursing
Faculty of Nursing, Ain Shams University
Dr. Camelia Fouad Abdullah, Professor in the Surgical Internal Medicine Department, Faculty of Nursing, Ain Shams University
Dr. Mona El-Shazly Mahmoud, Head of the Administration Department, Faculty of Nursing, Ain Shams University
Dr. Buthaina Nader Sadiq, Lecturer in the Pediatrics Department, Faculty of Nursing, Ain Shams University
Dr. Samar Marzouk, A lecturer in the Surgical Internal Medicine Department, Faculty of Nursing, Ain Shams University
Dr. Dina Mohamed Mohamed A lecturer in the Surgical Internal Medicine Department, Faculty of Nursing, Ain Shams University
Dr. Sarah Fathi A lecturer in the Internal Surgical Department, Faculty of Nursing, Ain Shams University
Review and supervision
Dr. Kawthar Mahmoud Mahmoud, Head of the Central Administration for Nursing
Prof. Dr. Hisham Atta Youssef, Assistant to His Excellency Prof. Dr. Minister of Health and Population
For human resources development and training
Prof. Dr. Sherif Wadih, Advisor to His Excellency Prof. Dr. Minister of Health and Population
For emergency
Dr. Nevin Abd Rab Al-Nabi Muhammad, General Director of Therapeutic Nursing Department
Dr. Ali Abdel Azim, Director General of Quality Management, Ministry of Health and Population
- Introduction
Nursing is a profession with a long tradition and history that extends to the spread of creation and represents the backbone of health care. Nursing administration represents a large component of the number of health team members working in the health care sector. The nursing team is an important element in this team because of the preventive services it provides. Therapeutic and educational .
The nursing team performs many vital roles by developing and implementing the necessary nursing plans for the patient, then continuously evaluating and educating the patient about health.
Therefore, we must update the nursing staff guide system, which links modern thought to the use of nursing information and its applications to improve the performance of nursing staff in hospitals and their performance in the burns department, especially so that patients feel satisfied with the care provided and the good use of available resources and the nursing staff’s feeling of job satisfaction through scientific clarity. And the technician for all nursing procedures. This modernization and development stemmed from the interest of the Ministry’s nursing leaders in developing and raising the efficiency of nursing staff members.
In order for the nursing team to perform optimally, it was necessary for them to fulfill their rights and duties through the laws and decisions issued by the Ministry of Health to regulate the work and to be familiar with the ethics of the profession and the administrative and technical systems of work procedures.
Vision of nursing serviceIn hospitals
The Central Nursing Administration is looking forward to improving the nursing profession and nursing services in hospitals in the Arab Republic of Egypt so that they can compete at the regional and international levels .
Nursing service message in hospitals
The Central Nursing Administration is committed to following up on the management of nursing services to raise the health level of individuals, whether sick or healthy, and to provide the best nursing services to all patients who need them in a way that ensures cost effectiveness and is in line with Objectives of hospital procedures and nursing administration, as well as working to raise the scientific and practical level of nursing staff members and change their attitudes towards modern trends in nursing and medical sciences .
Objective of the guide:
Establishing work systems in burn units ◼️
Confirming the efficiency of performance of nursing staff members ◼️
in burn units
Improving the scientific and technical level of nursing staff working ◼️
in burn units
Protecting burns unit workers from the risks expected in the unit◼️
Ensuring the safety of patients while they are in the unit◼️
- Introduction to burn units
Burn units are the appropriate place to treat critical cases under the supervision of an integrated team of workers who have the appropriate technical and personal experience that allows monitoring all minute vital changes in the patient while developing a protocol to improve survival rates while reducing infection rates and shortening the length of stay in the hospital .
Definition of burn unit
It is a unit where treatment beds are used for patients who suffer from major skin burns.
It is also the appropriate place to treat critical burn cases
It has an integrated team that provides nursing service at the highest
level for 24 hours
The number of nursing staff is fixed during the three shifts
It contains all the precise devices that the patient may need
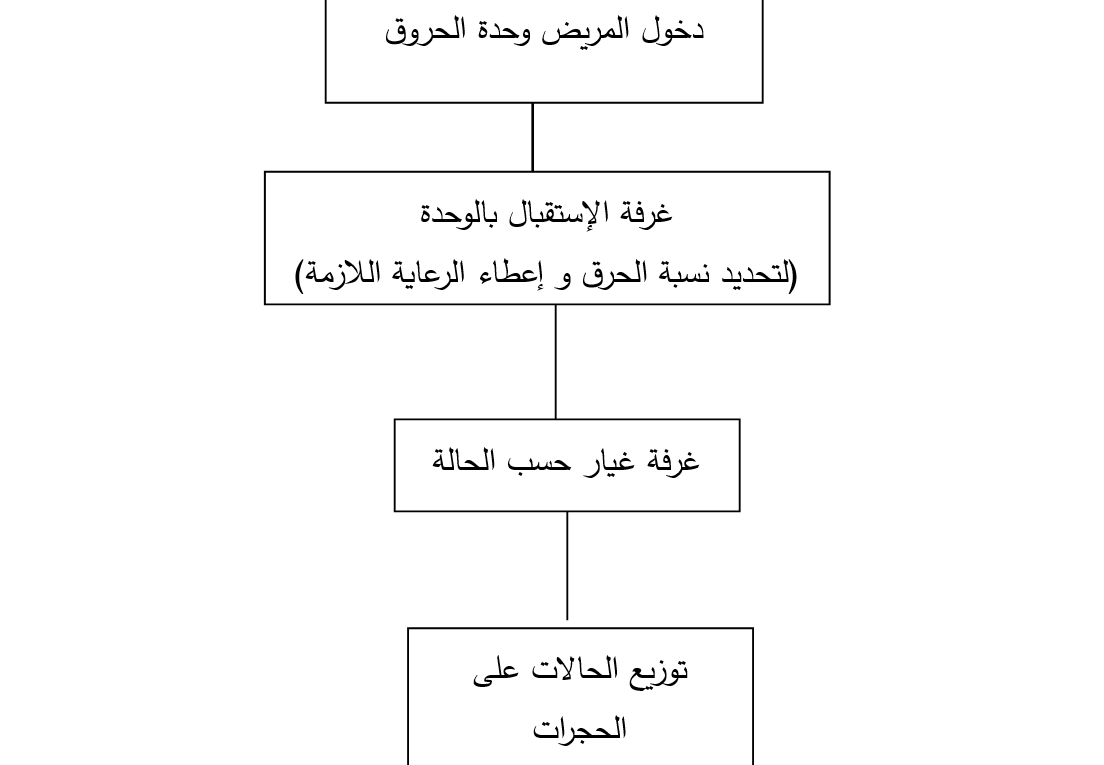
Components of the burn unit:-
1- Patient room (patient reception)
2- Dry changing room
3- Water changing room
4- Physical treatment room (powder bed)
5- The central station for nursing staff
6- The laboratory, to carry out the most important analyzes within 24 hours, the most important of which are:
- Gases in the blood
- Enzymes in the blood
- Sodium, potassium, calcium
- Uremia and creatinine in the blood
- Liver functions
- Blood sugar
- Cholesterol in the blood
7 - Store (medicines, supplies, furnishings)
Emergency trolley
|
First drawer |
the number |
Morning time |
Evening period |
Sleeping period |
|
Adrenaline |
5 |
|
|
|
|
lasix40 mg |
5 |
|
|
|
|
Dopamine |
5 |
|
|
|
|
Depotrex |
5 |
|
|
|
|
Noradrenaline |
5 |
|
|
|
|
Aminophylline |
5 |
|
|
|
|
Trideal |
5 |
|
|
|
|
Calcium |
5 |
|
|
|
|
Magnesium sulfate |
5 |
|
|
|
|
Soyum bicarb |
15 |
|
|
|
|
Potassium chloride |
10 |
|
|
|
|
Coradaron |
10 |
|
|
|
|
Solio Cortef |
5 |
|
|
|
|
Isopten |
5 |
|
|
|
|
Inderal |
5 |
|
|
|
|
Epanutin |
5 |
|
|
|
|
Xylocaine vial |
1 |
|
|
|
|
Dormikum |
5 |
|
|
|
|
Second drawer |
the number |
Morning time |
Evening period |
Sleeping period |
|
Syringe 10 ml |
10 |
|
|
|
|
Syringe 5 ml |
10 |
|
|
|
|
3 ml syringe |
10 |
|
|
|
|
There were no measurements |
10 |
|
|
|
|
Gauze bandage |
3 |
|
|
|
|
Blaster |
1 |
|
|
|
|
Sterile gel |
1 |
|
|
|
|
Tongue depressor |
1 |
|
|
|
|
IV device |
10 |
|
|
|
|
Blood transfusion device |
10 |
|
|
|
|
Syringe 20 ml |
10 |
|
|
|
|
Syringe 50 ml |
5 |
|
|
|
|
Rail syringe |
5 |
|
|
|
|
Latex glove box |
1 |
|
|
|
|
Intravenous connection |
5 |
|
|
|
|
Arterial connection |
5 |
|
|
|
|
Triple link |
5 |
|
|
|
|
Identification bracelet |
5 |
|
|
|
|
Laboratory tubes (various) |
10 |
|
|
|
|
Sterile gaskets |
10 |
|
|
|
|
Heart drawing paper |
1 |
|
|
|
|
Electrode bag |
1 |
|
|
|
|
Third drawer |
the number |
Morning time |
Evening period |
Sleeping period |
|
Laryngoscope |
1 |
|
|
|
|
Laryngeal tubes (sizes) |
10 |
|
|
|
|
Air passage (sizes) |
5 |
|
|
|
|
Ampoubag Mask (Sizes) |
5 |
|
|
|
|
Oxygen mask (adults - children) |
5 |
|
|
|
|
Nebulizer mask (adults - children) |
5 |
|
|
|
|
Nasal catheter for oxygen |
5 |
|
|
|
|
Extra batteries |
4 |
|
|
|
|
Fourth staircase |
the number |
Morning time |
Evening period |
Sleeping period |
|
Gastric tube (rail) sizes |
5 |
|
|
|
|
Urinary catheter (sizes) |
5 |
|
|
|
|
Suction catheter (sizes) |
5 |
|
|
|
|
Urine collection bag |
5 |
|
|
|
|
Chest tube + jar |
1 |
|
|
|
|
I wanted a steriliser |
1 |
|
|
|
|
Sterilized scissors |
1 |
|
|
|
|
cvp catheter |
2 |
|
|
|
|
Guide wire for cvp |
1 |
|
|
|
|
Silk thread |
5 |
|
|
|
|
Surgical scalpel |
10 |
|
|
|
|
Betadine 10% (bottle) |
1 |
|
|
|
|
A box of alcohol swabs |
1 |
|
|
|
|
Astray iPad |
1 |
|
|
|
|
searchlight |
1 |
|
|
|
|
Fifth staircase |
the number |
Morning time |
Evening period |
Sleeping period |
|
9% salt solution |
5 |
|
|
|
|
Ranger |
5 |
|
|
|
|
Glucose 5% |
5 |
|
|
|
|
Glucose 10% |
2 |
|
|
|
|
Glucose 25% |
2 |
|
|
|
|
Histril |
2 |
|
|
|
|
Hemagel |
2 |
|
|
|
|
Mannitol 20% |
2 |
|
|
|
|
on the roof |
the number |
Morning time |
Evening period |
Sleeping period |
|
Electric shock device |
1 |
|
|
|
|
Pressure device |
1 |
|
|
|
|
Earphone |
1 |
|
|
|
|
Large ampobag |
1 |
|
|
|
|
Small ampoubag |
1 |
|
|
|
|
CPR board )) |
1 |
|
|
|
|
Oxygen cylinder |
1 |
|
|
|
|
Solution holder |
1 |
|
|
|
|
List of high-risk medications |
1 |
|
|
|
|
A list of drug names that are similar in appearance and pronunciation |
1 |
|
|
|
|
the signature |
|
|
|
|
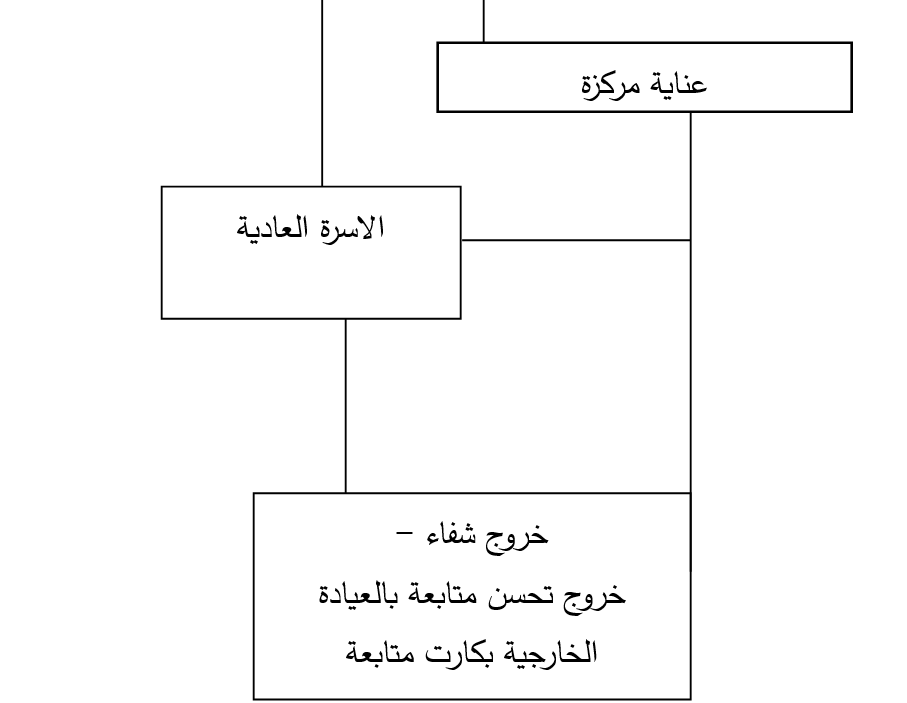
The patient enters the burn unit
- Job Descriptions
The Definition
It is a list that includes a group of elements specific to a specific job, such as [the name of the job, a summary of the job, the supervision of others over the job and the job’s supervision over others, duties and responsibilities, and the special qualifications to hold this job.
It is statements that explain the nature of the job and the responsibilities assigned to the job holder, as well as the relationship between the job and other jobs.
The job description of a health worker specifies:
· His powers, that is, his right to make decisions.
· His responsibilities are the amount of work that he is expected to accomplish.
Purpose of the job description:
It is to specify to the worker, the rest of the team members, and the supervisors:
· What the worker is expected to accomplish.
· The level of performance expected from him.
· In front of who is responsible?
· The people he supervises.
Contents of the job description:
Job name :
It is the official name of the recognized job for the person who does the work or performs the job, for example, nursing technician or nursing specialist.
The Date :
History is mentioned because the job description is not permanent. Employees and their duties change, and the job description must be reviewed and changed when necessary.
Job Summary:
Summarizes the main responsibilities of the job:
Duties:
These are the most important elements of the job description, and even the most important part of it, and each unit duty should be fully defined as a recognized part of the job holder's work.
Relations :
This is simple data related to the following
The title of the person responsible for the job holder in performing his duties.
Titles of the people whose work the incumbent supervises.
Qualifications:
The qualifications are described, including basic training
Principles of organizing and writing job description information:
· Arrange the description of duties in a logical manner.
· He mentions the separate duties clearly and concisely, and not going into detail becomes a motor analysis.
· Sentences begin with kinetic, functional verbs such as: perform, use.
· Use quantitative words whenever possible, meaning achieving the goal by 90%, for example. Using specific words whenever possible is better than unclear words.
· You start by mentioning the duties as duties and then delay the qualifications data.
· Avoid generalization.
· If possible, determine the percentage of the total position that is spent on activities.
· Limits the use of the word “maybe” in relation to the performance of certain duties.
· Using the daily, periodic, and sometimes routine, if defined well, will make the meaning more specific and clear.
Uses of job descriptions:
· Job descriptions are used in career guidance for new employees
· It is used as a basis for performance evaluation.
· Use job description items when making promotions.
· It can be used to identify weaknesses in performance.
· It is used to determine the numbers needed for work.
· It is used to determine or increase wages .
Job description card
|
Job title: Head nurse of a specialized unit |
Class: first - second |
|
Section: Burns |
|
Organizational relations:
Under the supervision of:
Director of Nursing at the hospital
Supervises: Burns unit nursing staff
Work's relationships :
Primary purpose of the job:
Determine the tasks of all individuals
Achieving the organization's goals
Improving individuals' performance
Improving the quality of nursing service
Roles and responsibilities :
1. It plans, organizes, and distributes work to the nursing staff in the unit
2. Estimating the unit's needs for nursing staff
3. It trains nursing staff and on-the-job training personnel, especially new ones or transfers, while motivating them to continue acquiring information and skills, and participates in their training.
4. Providing and completing the machines, tools and equipment necessary for nursing work
5. Prepares schedules for shifts, nights, rest, and vacations, and distributes work among nursing staff members
6. Supervising nursing staff members and following up on the implementation of nursing work by periodically visiting clinics
7. Supervising attendance and departure and related records
8. valuating the performance of the unit’s nursing staff
9. Assessing patients' nursing needs and developing unit nursing plans
10. Follow up on the implementation of treatment, observation, nutrition, and tests, and give directions to the nursing staff in the event of a deficiency or negligence in performance
11. Review registration and recording of files, records and patient tickets
12. Organizing meetings related to nursing work
13. She prepares a daily report on the condition of patients and the problems that obstruct nursing work, submits it to her direct superior, and follows up on the implementation of the observations thereon.
14. It suggests rewards and punishment
15. Training new members of the nursing staff, nursing students, and lower categories
16. Follow the rules and principles of infection control and ensure the quality of performance of various nursing tasks
17. She supervises the teaching and education of patients in the unit
18. Follows professional ethics and behavior in dealing with members of the health team, individuals, patients and their families
19. Carrying out similar tasks assigned to it
Job description card
|
Job title: Specialized unit nurse |
Class: second - third - fourth |
|
Section: Burns |
|
Organizational relations:
Under the supervision of: Burns Unit Supervisor
Supervises:
work's relationships :
Primary purpose of the job:
Determine the tasks of all individuals
Achieving the organization's goals
Improving individuals' performance
Improving the quality of nursing service
Roles and responsibilities :
Make patients' beds in the morning according to the patient's need.
Visiting doctors to see their patients
Implementing doctors’ orders, giving treatment, bathing the patient, changing clothes, and trustworthy food
You educate the patient about health
Follow the infection control system, write it down, and note vital signs as well as a fluid chart.
Performing the required tests and measuring blood sugar in the department (with a device trained by the department’s nursing staff).
Proper, complete and accurate recording and notation
Delivery and Receipt: (Patients, Equipment, Consumables)
Carrying out similar tasks assigned to it
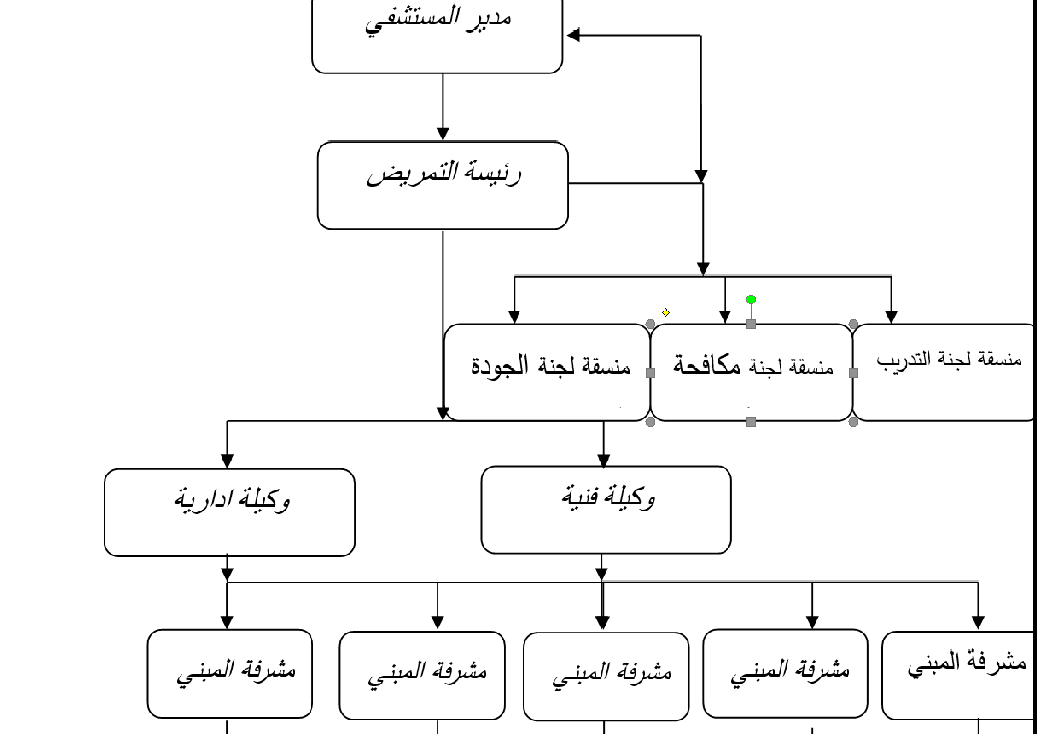
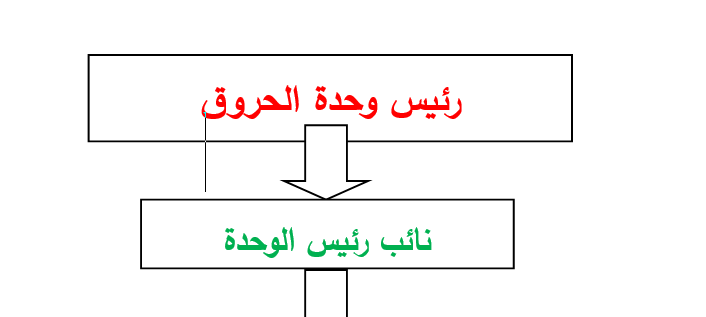
- Organizational Chart
The Definition
The organizational structure is the formal framework through which management takes its place through an illustrative drawing that defines relationships, through a description of the various centers that define the scope of responsibilities and authority, the scope of supervision, and the vertical and horizontal relationships between these divisions .
Types of organizational structure:-
- Formal organizational structure.
- Informal organizational structure.
Formal organizational structure:
The Definition
The formal organizational structure is defined by the executive authority as a result of planning. It draws and clarifies the relationship between people, their positions, responsibilities, and the relationship between them.
Informal organizational structure:
It includes personal and social relationships that do not appear in the formal organizational structure drawing.
Steps to prepare the organizational structure:
· Determine the purpose of the hospital.
· Determine the sub-goals necessary to achieve the goal.
· Determine the necessary activities and implement sub-goals. (Example: nursing/laboratory/nutrition activities...)
· Determine the work required to implement the activities.
· Grouping work into positions such as doctors/nurses/technicians/heads of units/specialties/supervisory/technical categories.
· Grouping jobs into sections, for example (nursing jobs).
· Grouping departments into departments and sectors and then grouping them under one executive body, such as the Directorate of Health Affairs/Treatment Institution/Health Insurance.
· Preparing an administrative organization guide that explains the rules, regulations, regulations and instructions, the most important of which is the organizational structure.
NB :
1 - The number of department supervisors is determined according to the hospital’s organizational divisions, according to the location of the departments, the number of beds, and the type of specialties .
2- The number of department heads is determined according to the organizational divisions of the different departments in the hospital .
3 - The number of supervisors, department heads, nursing staff members, and assistants in shifts and evening hours is determined for each hospital, according to the workload in each hospital .
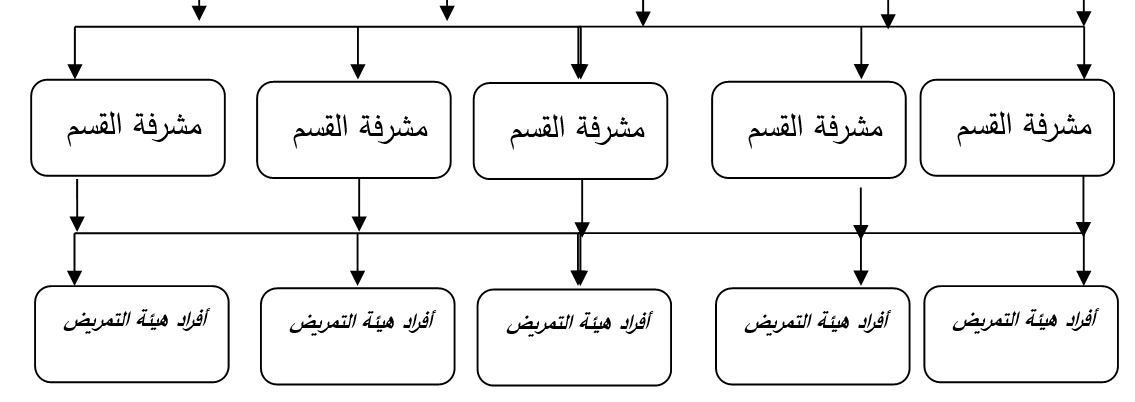
Organizational Chart
For the nursing department of a large general or specialized hospital
Organizational structure of the burns unit
Vision of the nursing service for the burn unit
The hospital's nursing administration looks forward to raising the professional level of nursing staff and providing nursing services to burns department patients effectively, safely, and with quality .
Nursing service message for the burn unit
The hospital's nursing administration is committed to raising the health standard of patients and providing them with the best nursing services in line with the objectives of hospital procedures and nursing administration. It also works to raise the scientific and practical level of all members of the nursing staff in the department and change their attitudes towards modern trends in nursing and medical sciences .
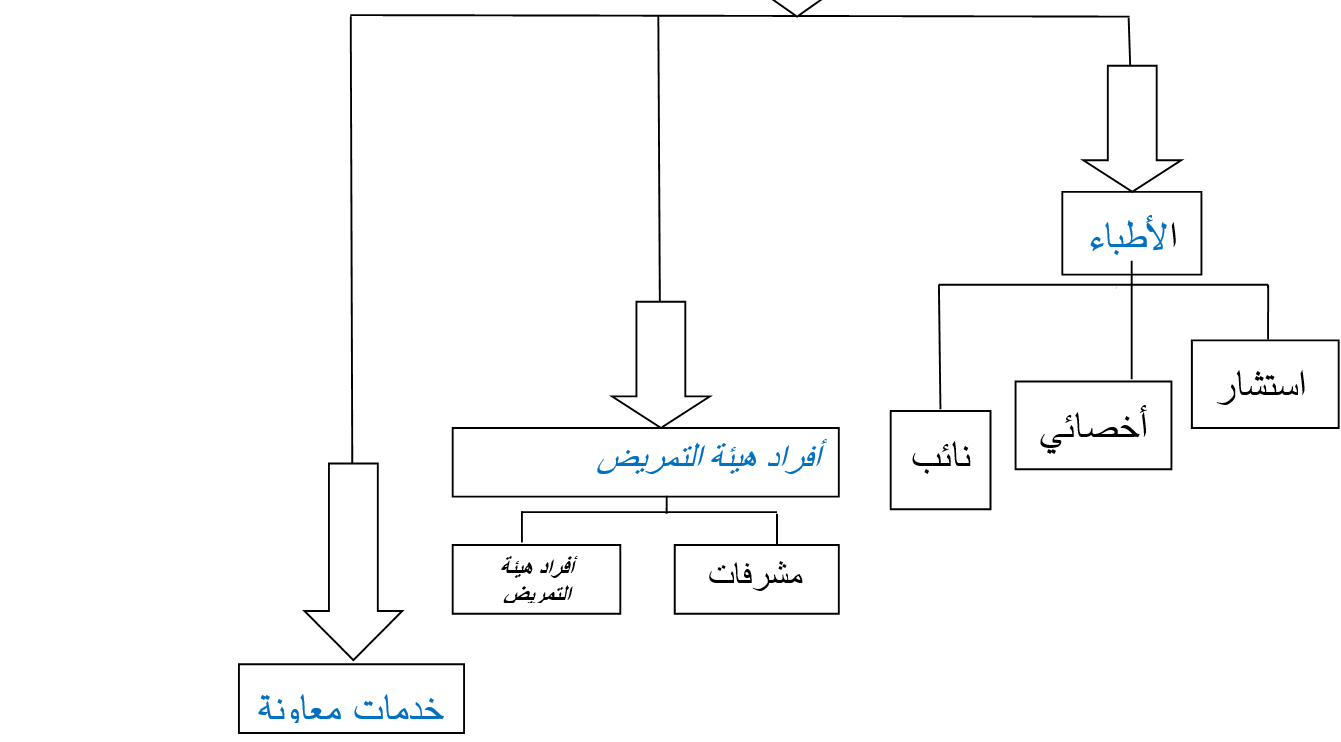
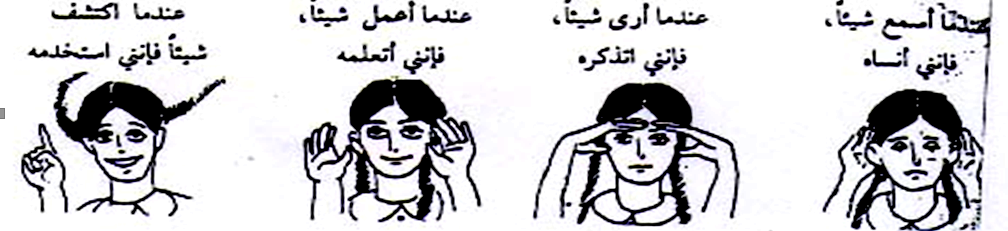
- Methods of communication
Definition of communication
Communication is the process of exchanging ideas, information, and trends verbally and non-verbally between individuals to achieve public or private purposes. Communication is a circular process and not a one-sided conversation . This means that the sender is at times a receiver and the receiver is at times a sender .
The importance of communication
• Forming relationships between community members.
• Exchange information, ideas and experiences.
• Conviction to change positive knowledge, attitude and behavior among individuals and groups
• Clarifying ideas, removing confusion, and correcting concepts .
• Increase culture.
• Influencing others through guidance and guidance.
• Transferring information, data, statistics and concepts through various channels to contribute to decision-making.
• A purposeful means to ensure interaction and joint exchange of the various activities of the organization .
• A way to motivate employees .
• Communication helps achieve goals .
Components of the communication
process:
• Sender
• The message
• Communication channel
• The future
• Feedback
• The environment
Types of communication:
1. Verbal .
2. Non-verbal.
There are two types of communication:
First: Verbal communication :
• Talk - printed material to read - watching a television or radio program
• Second: - Non-verbal communication:
• Body and hand movement - sitting - facial expressions such as joy and sadness - eye movement...etc
Communication skill:
1- Listening skill.
2- Speaking skill.
3- Persuasion skill.
4- The skill of asking questions.
5- 5 Dialogue management skill.
6- Skill in dealing with others.
7- The skill of using body language.
• Listening skill
It is focusing attention on the opinions, thoughts,
feelings, and linguistic and physical expressions of others. Do not rely
on the content of the words, but try to reach the speaker’s directions
The difference between listening and listening
◾ Listening : is limited to receiving the message organically through the ear .
◾ Listening : It is the use of the mind with its full capacity in everything that has been received, by processing the received message mentally with interpretation .
Types of listening:
Good listening is often accompanied by good thinking
Why don't we listen?
· Their inability to concentrate for any reason.
· Their intense preoccupation with themselves.
· They are so preoccupied with what they will say next.
· Their lack of confidence in what they are listening to and the reasons why they are listening to it
.
· They do not have the ability to follow the points that the speaker is talking about.
· They do not care about what is said to them.
· We think seven times faster than we speak, and this makes us preoccupied with our judgments about the speaker’s speech?
· Our desire to express ourselves instead of listening (I want the opportunity to talk).
· Distraction due to side conversations or noise..
The importance of good listening
Good listening is the appropriate path for a leader or individual with strong relationships with others, as it saves a lot of time and effort in managing problems and conflicts, achieving goals, and negotiating with those around them, as listening leads to :
· It affects the validity and accuracy of the decision
· It makes the relationship mature and strong between individuals
· Generates the ability to innovate and create
· It makes the individual able to face problems and crises
· It makes the criteria for evaluating others fairer
· Listening means a permanent addition to a person's ability to speak powerfully
· It reduces error and represents the key to safety for an individual’s intellectual growth.
How to become an effective listener?
· Look for the content of the topic and ignore the speaker's manner or mistakes in speaking.
· Arrange the information you hear logically in your mind.
· Do not rush to judge.... Rather, let the speaker finish his speech.
· Do not turn your face away from your interlocutor (the eye sometimes listens).
· Ask your interlocutor if the conversation is not clear.
· Create an appropriate environment for yourself from the beginning that prevents you from focusing on things other than listening to the speaker.
· Make your place in the session suitable for following the speaker with your eyes and ears, and try to eliminate factors that could obstruct this, such as sunlight falling on you or the presence of some devices in front of you
2- Speaking skill
How do you prepare yourself before starting the conversation?
· Determine the purpose and benefit of the communication
· Tailor your message to your listeners
· Good preparation of the topic of the conversation...it is the best source of trust.
· Have an idea in advance about the person you will be speaking to.
· Prepare supporting materials to support your talk.
· Mental and muscle relaxation.
To be a good speaker
· Avoid inexpressive faces - exaggerated expressions - distressed expressions.
· Avoid sharp glances or direct, close-up looks.
· Avoid repetitive movements as a result of excessive nervousness (movement such as a pendulum clock, for example).
· Avoid inappropriate or excessive clothing.
· Avoid stuttering - low voice - staying on one tone.
· Expand your circle of thinking and fully understand the information
· Use the recipient's language to convey the message clearly
· Ask questions and then let the speaker confirm that what you have understood is in fact correct
· Do not say lightly: I do not know: many of us know very little about the world in which we live, and pretending to answer or fabricating it only doubles the problems.
· Pay your full attention to those you talk to: If you set aside time to communicate with someone, give them attention and attention. Join the conversation and participate in it when you see that it is of interest to the communication process.
3- Persuasion skill
It is one of the skills necessary for the communication process, and it is used in personal interviews, group discussions, and talking with leaders. Definition: Enticement through reason, logic, and knowledge to make others accept changes in their opinions, attitudes, or behaviors.
Stages of the persuasion process:-
· Attention stage: The individual is attracted to the new idea and shows enthusiasm for this idea.
· Interest stage: A stage in which the individual wants to know details about the idea and has a desire to analyze facts and collect information.
· Evaluation or mental comparison stage: In this journey, the individual performs a process of self-evaluation and comparison between the old and the new.
· Experimentation stage: In this journey, the individual tries to get rid of tension and attraction, so he experiments and applies the pleasure of the idea on a small scale.
· Adopting the idea/complete conviction: In this journey, the person is completely convinced of the idea and decides to continue implementing it.
The skill of asking questions
To keep the dialogue going, there must be a reaction from the other party that includes indicators that support that it received the message and helps the first party determine how to continue the dialogue. These indicators can be obtained through the optimal use of questions. The questions may be positive or negative. If they are positive, they explain the other party’s way of thinking and feeling, but if they are negative, they make him feel tense and embarrassed and push him to take a defensive position.
Therefore, the following must be taken into account:
· The goal of questions should be to reach agreement and not get into personal matters.
· It is important not to ask questions that cause anxiety and tension to the other party.
· Questions should help both parties, not be used as maneuvering.
· Questions should aim to establish an atmosphere of cooperation by motivating the other party to respond frankly.
· Make sure that the questions are not deceptive, contrived, evasive, shameful, or worthless.
· Questions should be appropriate to the situation.
· The questions should also be appropriate to the personality of the other party and his general aptitudes.
· The purpose of questions should be to achieve a goal and not simply to elicit a response.
· There must be a connection between the questions.
· Finally, it is required and usual for questions to be characterized by tact and respect for the other party.
Specifications of successful communication:-
· Both the sender and the receiver must believe and be interested in the message
· 2. Mutual respect between sender and receiver
· The subject of the message is clear to both parties
· Use appropriate means for the sender, the recipient, the subject of the message, and the place where it is presented
· Communication is two-way, meaning there is interaction between the sender and the receiver
· Use verbal and non-verbal communication equally efficiently as they complement each other
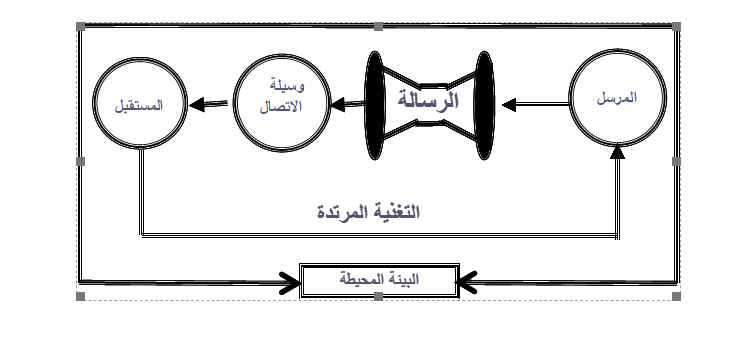
· The more senses we use, the more efficient the communication process becomes
· The message must be correct, accurate, clear, specific and short
· Do not be a constant sender or receiver
· Set a clear goal for the communication process
· Choose the appropriate circumstance from an environmental, social and psychological perspective
· The language of communication must be appropriate for both parties
Specifications of successful communication
· Both the sender and the receiver must believe and be interested in the message
· Mutual respect between sender and receiver
· The subject of the message is clear to both parties
· Use appropriate means for the sender, the recipient, the subject of the message, and the place where it is presented
· Communication is two-way, meaning there is interaction between the sender and the receiver
· Use verbal and non-verbal communication equally efficiently as they complement each other
· The more senses we use, the more efficient the communication process becomes
· The message must be correct, accurate, clear, Specific and short
· Do not be a constant sender or receiver
· Set a clear goal for the communication process
· Choose the environmentally appropriate condition, Social and psychological
· The language of communication must be appropriate for both parties
Basic principles for communicating clearly
In order for people to hear, see and understand the message you want to deliver to them, you must:
Choose words that are easy and simple to understand.
To avoid scientific and medical terminology.
Make sure that everyone present sees and hears what you are saying.
To present a message as short as possible without disturbing the content of the message.
Long messages lead to the attendees being distracted and not focusing on what you are saying and presenting. It also leads to them not remembering the message shortly after your speech.
You should talk to them about one topic at a time.
- Ethics and ethics of the nursing profession
First: Duties and responsibilities of the literary profession :
There are moral duties and responsibilities that govern and regulate the work of the nursing profession, in addition to the professional responsibilities and duties of nursing staff members. All organizations interested in the nursing profession, most notably the International Council of Nursing Staff, have paid attention to them, stressing the need for nursing staff members to adhere to the morals and ethics of the nursing profession. Therefore, it has drawn up a constitution and a code of ethics for the profession so that nursing staff members can be Nursing is aware to emulate and implement it, which will have an impact on the positive image of the nursing staff in society and their emergence as role models.
The most important provisions of this constitution are the following :
· Respecting life, alleviating suffering, and working to alleviate pain and raise the level of health.
· Providing the highest level of nursing service and professional behavior.
· To be prepared to practice the profession only and to work to acquire information and skills.
· Respect the patient's religious beliefs.
· Keep all information she obtains through her work and do not disclose it except in accordance with the law.
· Do not prescribe or give medical treatment without a doctor’s orders, except in emergency cases and notifying the doctor immediately.
· She is committed to carrying out the doctor’s orders intelligently and obediently, and refuses to participate in any unethical actions .
· Gain the trust of the doctor and health team members.
· Not allowing their names to be used in advertising products or in any form of personal advertising.
· Cooperating with members of other professions and with her nursing colleagues.
· Adhering to the standards of personal etiquette in her private life.
· Citizens and members of other health professions participate in their efforts to meet the health needs of the local, national, and global community.
Thus, the nurse has many responsibilities and duties towards the patient, herself, her colleagues, her workplace, society, and her profession in which she works.
The following are the most important ethical responsibilities of nursing staff members:
The most important responsibilities of nursing staff towards their patients are:
· To keep in mind that healing the patient and preserving his health is their primary goal, without other considerations such as religion, color, gender, or politics.
· To be the place of trust placed by the patient in terms of his recovery.
· To be kind-hearted in their treatment, to act wisely and accurately towards their patients, to give the patient hope for recovery, whether physical or psychological, to maintain absolute confidentiality of everything you know about the patient, and to participate with the patient in making some decisions related to his treatment.
· They should be responsible for health education for the patient and providing him with complete information regarding his illness, how to cope with it, and what are the means of avoiding complications resulting from it, and not just giving him medication .
Responsibility of nursing staff towards themselves:
· Nursing staff members must work to improve their scientific level by constantly being informed of everything new in the general natural sciences and special nursing sciences.
· Completing studies to obtain available academic degrees such as a specialized diploma, master’s and doctorate.
· Attending seminars, scientific conferences and seminars organized by medical and nursing societies and participating in scientific research that helps advance the nursing and health care profession.
· To be fully convinced of the nursing profession and to bear in mind that this profession has its own respect, dignity and dignity, and to be of good conduct and behavior in their public and private lives.
Responsibilities of nursing staff towards their colleagues at work:
· Sincere cooperation with members of the health team, which helps provide health care to citizens.
· They treat their co-workers as they would like to be treated and avoid talking badly about them and any comment or remark that would detract from the skill or opinion of any co-worker.
· Fully prepared to teach recent graduate colleagues all the foundations and concepts of modern nursing.
Responsibility of nursing staff towards the institution in which they work:
· Respecting the organization’s work laws and rules.
· Respect all employees of the organization and cooperate with their superiors.
· Respect the full uniform while working.
· Proper use and preservation of work tools, and reporting in the event of loss or damage to any of the devices and tools.
· Admitting the mistake and reporting it to those concerned.
The nurse's responsibility towards society:
· To be good citizens who respect the traditions and customs of society.
· Not participating in work that affects the honor and dignity of citizens.
· To be sufficiently familiar with the laws and legislation of the state.
Responsibility of nursing staff towards the nursing profession:
· Paying attention to their appearance, adherence to dress, cleanliness and grooming.
· Stay away from any action that raises suspicions around her and have good behavior.
· They must be convinced of the profession and that it is a humane work that is respected.
· Raising the level of the scientific profession through scientific research while delivering information to other groups.
· Working to improve the physical, economic and social conditions of workers in the profession
· Improving the level of performance of nursing services in their workplace, as well as improving the selection of workers.
The following are the most important qualities necessary for nursing staff members:
1- Nursing staff members must possess the most beautiful qualities that qualify them to carry out their mission in the best way, such as:
2- Healthy body and mind .
3- Be mature in thinking and acting.
4- They have basic information about the profession as well as general information.
5- They have skills specific to the nursing profession.
6- They have the ability to gain the trust of others and teach others.
7- They have sound attitudes towards their profession.
8- Role models in their cleanliness and good appearance.
9- A Strong observation and smart people.
10- To be firm.
11- Conscientious and cooperative .
12- His ability to make decisions and have emotional stability, especially in crises and critical situations .
13- Quick intuition and quick action.
14- Self-confidence.
Patients' rights
1. The availability of policies and procedures that define at least the following patient rights :
· The right to receive care if it is available in the hospital.
· The right to know the treating physician, supervising physician and/or physician Administrator .
· The right to receive care that respects the patient's personal values and beliefs.
· The right to know and participate in decisions regarding their care.
· The right to refuse care and not continue treatment.
· The right to security, personal privacy, confidentiality and dignity.
· The right to receive appropriate treatment for pain.
· The right to file a complaint or suggestion without fear of persecution.
· The right to know the prices of services and procedures.
2. Patients' rights must be clear and announced to patients and the staff.
3. The availability of policies and procedures that define patient duties, which include, at a minimum, the following:
· Follow hospital policies And its procedures.
· Financial commitment in accordance with the law, regulations and hospital policy.
· Show respect for other patients and healthcare workers .
· Follow the suggested treatment plan .
4. Availability of policies and procedures to inform patients and their families of their rights and duties regarding refusing or not continuing treatment.
5. Availability of policies and procedures that specify the process for patients to submit complaints or suggestions verbally or in writing without mentioning their names.
6. Availability of policies and procedures that define the process of obtaining a statement of consent based on patient identification, and specify the validity period of signed consent before obtaining new consent.
7. The availability of a written form in the event that the patient’s belongings are delivered to a relative, containing the name of the person to whom it is delivered, the national number, the signature of the recipient, and the person responsible for the delivery.
8. The hospital has a list of procedures or types of treatment that require patient-identified consent, which includes the following:
· Surgical interventions.
· Anesthesia / general or hemiplegia.
· Transfusion.
· High-risk procedures or treatment (including but not limited to electrotherapy, radiotherapy, chemotherapy).
· Family planning interventions.
· Research.
9. The hospital has a system for informing patients and their families about available services and how to obtain them.
10. The hospital has a system in place to inform patients and their families of any expected costs.
11. Availability of a policy that specifies the hospital’s responsibilities towards the patient’s belongings, including at least the following:
· who is in Charge .
· When does responsibility for these belongings begin?
· How to protect belongings.
12. There is a specific process for informing patients and families about the results of care and treatment.
13. Availability of policies and procedures that specify how the hospital informs patients and their families about how to donate organs and other tissues.
14. Availability of policies and procedures that define the autopsy process and document the results of this process.
Rights of nursing staff
The purpose :-
Informing nursing staff of their rights and assisting in fulfilling them.
Steps:-
The hospital administration determines the general rights of nursing staff members in coordination with the Nursing Services Administration, which include the following:
1- The worker’s right to feel that the hospital needs him.
2- The right to feel part of the hospital.
3- The right to feel that work relations are good.
4- The right to feel respect and dignity
5- The right to know (to understand the hospital’s goals and policies)
6- The right to feel responsible.
7- 7 The right to complain .
8- The right to feel equal rights without favoritism or favoritism toward some at the expense of others .
9- The right to an agreed upon written list of rewards and penalties.
10- The right to continuous training during working hours .
11- The right to a system of encouragement and motivation, materially and morally .
12- The right to free health care and proper nutrition .
13- The right not to discriminate between categories of workers in the employment treatment system .
14- The right to a system of entertainment, psychological, social and cultural care .
15- The right to a system to prevent and protect against disease .
Duties of nursing staff towards their patients
· To keep in mind that healing the patient and preserving his health is their primary goal, without other considerations such as religion, color, gender, or politics.
· To be the place of trust placed by the patient in terms of his recovery.
· To be kind-hearted in their treatment, to act wisely and accurately towards their patients, to give the patient hope for recovery, whether physical or psychological, to maintain absolute confidentiality of everything you know about the patient, and to participate with the patient in making some decisions related to his treatment.
· They should be responsible for health education for the patient and providing him with complete information regarding his illness, how to cope with it, and what are the means of avoiding complications resulting from it, and not just giving him medication
- Quality
Definition of quality:
Definitions of quality vary depending on needs and habits, and these definitions may apply to many services. Therefore, there are many definitions of quality, as follows:
◼️ Quality is judging a specific thing based on specific specifications or conformity with needs and specifications.
◼️ Quality is doing the right thing in the right way.
◼️ Quality health care is the application of medical science and technology in a manner that achieves the maximum benefit for public health without exposure to risks.
Different dimensions of quality:
◼️ Effectiveness and impact : The more effective the service is, the more it can be described as being of high quality.
◼️ Efficiency: meeting societal requirements.
◼️ Professional empowerment of workers to provide the service.
◼️ Ease of access to the service: ensuring benefit from resources and achieving fair distribution of the service to the community.
◼️ The relationship between people: whether between workers and each other or between beneficiaries of the service.
◼️ Continuity: to ensure continued use of the service to reach a high level of quality.
◼️ Resources: Providing what is necessary to provide care so that it is an integrated service.
Quality assurance :
Quality assurance in the field of health services is the application of standards in a safe and acceptable manner to the community and at an acceptable cost, such that it leads to an impact on the incidence of disease rates, mortality rates, disability,
and malnutrition.
Quality assurance principles:
There are four principles for quality assurance, which are as follows :
1- Focus on client/beneficiary services: Service planning must depend on the needs and desires of the client or beneficiary, and there are two types of beneficiaries: internal and external.
(a) Internal beneficiary:
They are those individuals within the business who depend on each other to provide the service. An example of this is service providers, supervisors, and the rest of the team.
(b) External beneficiary :
He is the beneficiary of the service, such as the patient or the community .
2- Focus on the system or processes (procedures):
Processes are defined as a successive set of steps or tasks that transform people, methods, and materials into products or services. These operations are implemented within a system, where the system is defined as a group of interconnected operations. Quality problems may result in one process as a result of a deficiency in one or in several other processes belonging to the same system, or resulting from a failure to coordinate these interconnected processes. If the processes are incomplete, then the outputs will also be incomplete. Therefore, improving quality requires an understanding of processes and acceptable levels of their variation.
3- Focus on information-based decisions:
Information in the organization is like blood in the human body, so it must be accurate and timely, which ensures the correctness of decisions. Information is particularly needed in places that suffer from problems because of its importance in the following:
(a) Define the problem
(b) Identify the causes of the problem or the processes in which errors are expected to occur
(c) Measure the results of the solutions applied and ensure that they work correctly
4-Focus on participation and the work of quality improvement teams:
All employees must participate in implementing the correction plans resulting from the application of quality improvement steps, and this has advantages including the following:
(a) Workers have a more accurate sense of the errors that occur in their work and the best way to correct them
(b) Employees prefer to implement changes that they feel involved in decision-making.
The difference between quality assurance and quality improvement
There are three basic differences between quality assurance and quality improvement as follows:
1- The quality assurance system relies on quality control by reviewing patient files and verifying the implementation of treatment according to sound scientific foundations, then identifying deficiencies or errors and determining methods for correction, while quality improvement focuses on preventing errors before they occur.
2- The quality assurance process leads to accusing those who made a mistake and raising strong sensitivities among employees, while quality improvement focuses on increasing cooperation and participation among employees, which leads to determining the correct path to avoid mistakes.
3- Quality assurance processes are always carried out separately from administrative development, while the proper application of quality assurance achieves the integration of the two processes together, which leads to achieving the desired goals.
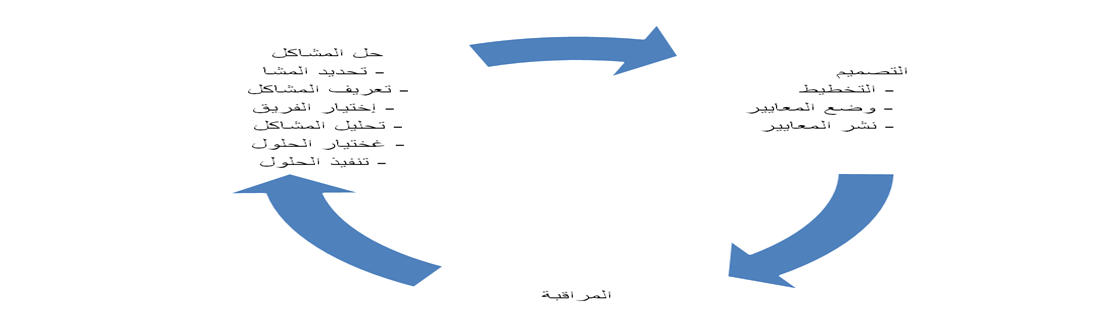
Quality assurance process
The quality assurance process includes steps that came as a result of many experiments and are called the steps of the quality assurance program or elements of quality assurance, and sometimes it is called the quality assurance cycle or quality improvement cycle. Whatever the title, this course includes three groups of activities, as in the following figure, Figure (1):
Figure (1)
Standards
Standards constitute a very important part of any quality assurance program at the levels of the organization. It is not enough for the organization to be aware of the dimensions of quality on which the quality of the services provided depends or to judge them, but rather the organization must help those who work in it to achieve the client’s expectations accurately by setting the standards for them. Which makes this easier for them.
The Definition:
The standard is a definition of expected quality, and its goal is to ensure that the service matches the needs and expectations of the customer and not the needs and expectations of the hospital.
Standard characteristics:
1- Credibility: means that there must be a strong relationship between the standard and the desired results, and that the standards be based as much as possible on research evidence.
2- Reliability (stability): means that the standard always gives the same results every time it is used under the same measurement conditions.
3- Realism: means the possibility of using standards within the resources available to the organization.
4- Clarity: The standards must be understandable to those who use them.
5- Modernity : The standard reflects the latest scientific information available.
Standards sources:
There are many sources of standards, some standards have been previously prepared, and sometimes it may be necessary to prepare new standards, as follows:
◼️ Standards previously prepared:
o Local standards.
o International standards.
o Standards from service bodies and institutions.
o Standards from educational institutes and institutions.
o International experts.
o Local experts.
◼️ Standards being re-established:
Sometimes it may be necessary to prepare a new work manual and prepare updated specifications. In such a case, there are many sources that can be relied upon, such as:
o The World Health Organization and other international organizations.
o Professional bodies such as unions and scientific societies.
o Educational institutes.
o Global experts.
o Local experts.
Nursing standards:
They are acceptable and honest definitions that express the quality of nursing care. Standards are not considered valid unless they have a means of measurement so that they are given the opportunity to measure the quality and effectiveness of nursing care.
Nursing standards have been set by multiple institutions concerned with the quality of nursing care, and these standards differ depending on the institution, as some consider the standards to be the minimum required level of service. Whatever the definition, the function of the standard is to provide the means by which the level of quality is measured.
Writing nursing standards:
In order to write nursing standards, seven steps must be followed as follows :
1- Choose the specialization that will be covered by the standards and type.
2- Determine the goal of setting standards and specify the purpose of achieving them if:
· Patient focused
· Focuses on the nurse
3- Determine the nursing actions necessary to achieve the goals.
4- Determine the time needed to complete nursing work.
5- The standard is written in an acceptable form.
6- Review each standard, taking into account that there are no ambiguous words or actions that are difficult to measure.
7- Measuring the availability of standards-specific characteristics in each standard that has been developed
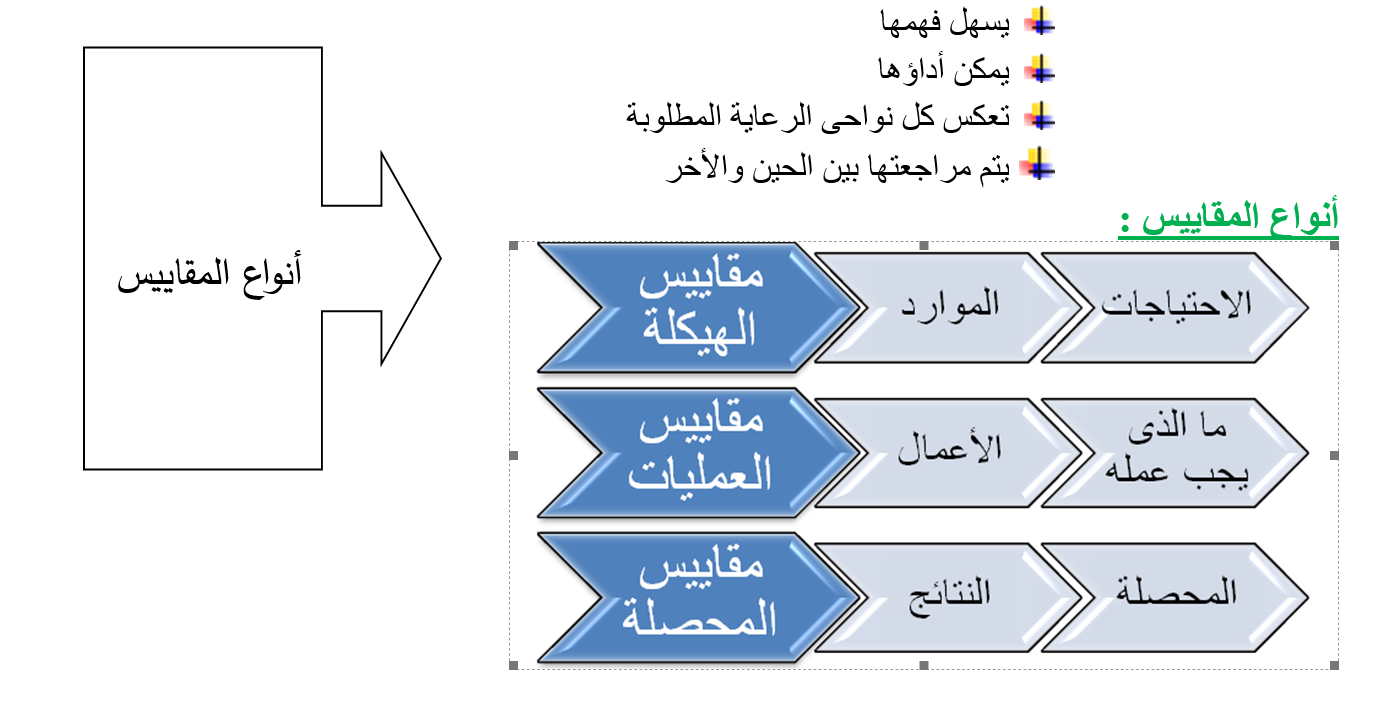
Measurements
The Definition :
The standard is a statement that describes performance and behavior, and expresses the academic or skill state that represents the positive level required for the thing. Standards are indicators of standards, and must be specific to a particular specialty or patient care.
Scale characteristics:
The standard must have:
· A detailed index of the standard
· Specific to a particular specialty or type of patient
· It can be measured
· It contains elements:
Improving the work environment
Definition of Kaizen philosophy:
It is a compound word of two parts that means “change for the better,” and it is a primary means of achieving Continuous improvement includes many of the improvement tools used in management, and one of these tools is 5S.
It is the philosophy of taking care of the workplace by organizing and cleaning it. It consists of five basic steps and each step is named in Japanese with a word that begins with the letter S Hence the name 5S . This philosophy became known worldwide by this name, and these five Japanese words were even translated into English words starting with the letter S For the designation to be valid. We can translate these five words into Arabic words that begin with the letter T, which are classification, organization, cleaning, standardization, and stabilization.
The five elements of this philosophy:
Five T consists of five elements:
1 - Sorting classificationIn Japanese, it is Seiri :
Taking care of the workplace begins with classifying everything in it.
Meaning of classification: Classification here means that we classify things into things that are necessary for work at the present time and things that are not necessary for work. After that, we get rid of the things that are not needed for work and keep those that are necessary for work. Such as: tools, files, materials, waste, papers, and equipment.
The classification process is the first step in this process
2-Organizing Set in OrderIn Japanese, it is Seiton :
After that comes the organization process, which aims to preserve the things that we decided to keep in an organized way that helps us perform the work efficiently. The organization process does not only include arranging tools or files on the shelves, but it also leads to reconsidering the general plan of the workplace itself. We have to think about the most appropriate way to organize the workplace based on our current work.
3- Cleaning or ShiningIn Japanese, it is Seiso :
The goal is a very clean work environment. This process is a process that occurs periodically, every shift or every day. There are things that must be cleaned by the person who uses them or handles them, such as work tools, including keys, tools, and supplies that he uses.
4- StandardiseIn Japanese, it is Seiketsu :
After all this effort and experience in organizing and cleaning, specific rules should be established for what the workplace should be like. This includes defining the responsibilities of each individual, setting standard methods for the cleaning process, and announcing all of this so that each individual knows what duty he has on a regular basis and how to perform it. This ensures that the situation will continue in this good manner and we will not return to old habits again.
5-Install SustainIn Japanese, it is Shitsuke :
We come to the final step, which is establishing systems to ensure the continuity of this entire process. For example, systems are put in place to review the cleanliness of places. An effective method is for one party to inspect another party, and a representative from one department inspects the process of filing files in another department or the cleanliness of the work site.
Five benefits:
There are many benefits including:
1- Reducing time wasted searching for documents or tools .
2- Reducing injuries due to the cleanliness of the floors, the absence of anything lying here and there, and the clarity of safe passage places .
3- Reducing equipment malfunctions due to their early detection.
4- Eliminate excess effort and unnecessary movements through the process of serious organization .
5- Feeling a beautiful work environment as a result of the cleanliness and organization process .
6- Replace damaged tools as soon as they are damaged, instead of discovering it late and disrupting work .
7- Discover lost things easily .
8- Reducing the malfunctions that occurred after maintenance operations as a result of some dust entering the delicate components (and this has been mentioned in other fields) .
9- Reducing quality problems that occurred due to pollution and dust.
- International standards and goals for patient safety and security
The Definition
A common goal that requires the process of coordinating the efforts of the health staff with the patient to protect him from injuries. A process provided by the institution to make the health care provided more advanced, safe and secure. The process of preventing unexpected patient injuries.
Principles and standards of patient safety and security:
Risk assessment: environment - patient .
Identifying risks: - developing a plan to protect the patient - how to act when an error occurs - recording and analyzing the incident -
Determine the cause - develop solutions to reduce the reoccurrence.
Who is responsible for the patient's security and safety?
Patient safety and security standards are the right of every patient and the responsibility of all employees of the medical institution.
No employee is excluded, regardless of their administrative responsibilities:
Senior management, department managers and employees
Patient safety and security standards:
1. Introducing the patient in the correct way.
2. Improving good and effective means of communication.
3. Safety of using high-risk medications.
4. Ensuring the operation, the correct procedure, and the correct patient.
5. Reducing the risk of infection by washing hands.
6. Reducing patient falls to prevent injuries.
7. Preventing disconnection or misconnection of catheters or tubes.
8. Preventing bed sores.
1- Risk management and patient safety.
10. Delivery and pickup policy.
11Isolation and restriction policy.
First criterion:
1. Introducing the patient in the correct way:
Failure to introduce the patient in the correct manner leads to:
· Giving the medicine to another patient.
· Performing a procedure on another patient.
· Delaying giving treatment or performing a procedure.
· Giving an incorrect diagnosis.
· Connecting a wrong patient to operations .
· Cancel an operation.
Why does an error occur in the definition?
· Multiple interventions.
· Multiple places to provide the service.
· Multiple individuals dealing.
· Some patients are unable to identify themselves.
· Lack of a clear definition system.
How do we avoid identification errors?
· Don't worry - take the time.
· Do not depend entirely on the patient.
· Make sure the information, stickers, and identification bracelet are correct.
Do the following:
· Introduce the patient in the correct manner upon entry.
· Make sure the patient's name is as it appears on the ID card.
· Make sure the identification data is correct before putting it on.
· Put on a new bracelet if you lose the old one.
· Ensure that the patient complies with the required procedure.
· Ensure that the patient is properly matched before transferring him.
· Apply a sample identification label immediately after taking the sample and before leaving the patient.
Do not do the following:
· Do not dictate to the patient His name, but let him tell you his name.
· Do not take any sample before matching the patient with the data on the sample request form.
· Do not label the sample identification on the container before taking the sample.
· Do not complete the work of the procedure remotely.
Understand and adhere to hospital policy:
· The hospital’s commitment to international goals for patient safety and security :
· Patients are identified by their admission site.
· The hospital’s commitment to at least two definitions:
· Patient's name is quaternary.
· His medical code.
Both definitions are verified each time when:
· giving medicine .
· Sample collection.
· Giving blood or its derivatives.
· Do any tests.
· Take any other action.
Second criterion:
Improving effective communication methods.
The means of communication that most lead to errors:
· Verbal orders.
· Telephone orders.
Receiving test results verbally or by telephone.
Verbal orders: administered face to face between the sender and the receiver .
Telephone orders: administered through the telephone between the sender and the receiver .
Responsibility of the recipient of the message or order:
· Writing the order or message while dictating orally or by telephone.
· Read the matter to the sender and wait for a response with a comment.
· If the matter is related to giving medicine, it must include the five basics.
· After reading the order, the receiver completes the order data by writing the date and time, the recipient’s name and position, the sender’s name and position, and then signing.
· In emergency situations, such as a “cardiac arrest,” it is sufficient to repeat the command to the sender and wait for a response with feedback.
Responsibility of the sender or giver of the order:
· Sign the order quickly.
· Spell the name of the medication if necessary.
· The numbers are dictated as they are pronounced, then each number is mentioned separately.
· Gives the command without using the abbreviation.
v Understanding and adhering to hospital policy:
· The hospital accepts verbal and telephone orders within very limited limits when it is impossible to write them by the person responsible for them and if delaying them may affect the patient.
· The sender and receiver must abide by their responsibility in this regard.
· The sender's signature on the given order shall be made no later than 24 hours.
Third criterion
Safety of using high-risk medications.
Definition of high-risk medications:
These are medications that, if used in an inaccurate and improper manner, may lead to serious injury or death to the patient.
The most important of these medications are:
· Insulin.
· Narcotic medications.
· Anticoagulants.
· Potassium chloride KCl And potassium phosphate.
· Sodium chloride solution more than 0.9.
Why do errors occur and suggestions for preventing them?
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
· Develop and disseminate a bilateral review policy |
· Lack of bilateral review policy |
Insulin |
|
· writing“Unit”instead of U |
· Use the letter U Expressed as the number of units |
|
|
· They are placed in different and labeled shelves |
· Place the insulin container near the heparin container |
|
|
· Use self-programming or dual-review pumps |
· Incorrect programming of the solution pump |
|
|
· Coordination between them |
· Do not link insulin administration with meals |
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
· Limiting their presence to their designated places |
· Put them in the regular departments with the stock of other medicines |
Drugs Morphine |
|
· Develop and disseminate a narcotic drug policy |
· Lack of policy and procedure for its use |
|
|
· Preparing printed medical orders explaining what is used in cases of mild to moderate pain · * It is necessary to have a doctor in case of severe pain |
· Using verbal or telephone orders |
|
|
· Use a pain assessment form |
· There is no way to evaluate pain |
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
· Not to be placed in regular nursing departments |
· Presence in regular nursing departments
|
Potassium chloride And Potassium phosphate |
|
· the chapter Among them in storage and preservation places |
· Mixing the two medications |
|
|
· Unify focus |
· Do not put a sticker Dosage and quantity after preparation |
Anticoagulants (heparin) |
|
· Use single dose containers |
· Use multi-dose containers |
|
|
· Separation of the two medications |
· Confusion between heparin and insulin |
|
|
· Relating doses to laboratory results |
· Determine doses without relying on laboratory results |
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
o Limiting his presence to care - operations - pharmacy |
o Its presence in regular nursing departments |
Sodium chloride at a concentration of more than 0.9% |
|
o Develop and disseminate a bilateral review policy |
o Lack of bilateral review policy |
o General instructions to reduce the risks of giving medications in general:

· Passing the “drug review” test is a condition for allowing treatment to be given.
· The presence of a pharmaceutical reference for some medications.
· Develop a bilateral review policy by two nurses and circulate it.
· Linking the administration of some medications to laboratory results.
· link Giving analgesics by assessing pain.
· Delete the presence of high-risk medications from the sections.
· Lack of medicines with similar packages and similar taste in one place.
· Place a clear label with the name in the place where each medication is kept and stored.
· Review the use of a two-way solution pump.
· After administering the treatment for the first time, the medication label is compared - according to the medical order - to the medication administration record sheet. When administration is repeated, the medication label is compared to the medication administration registration sheet.
· Identifying, recording, analyzing errors and finding out the reason is the path to improvement.
Keys that help avoid errors when giving treatment:
· Information about the patient.
· Information about the medicine.
· Effective Communication .
· Labeling of pharmaceutical packages: Medicines with similar packages or with a similar sound must be prepared when preparing their packages. Each package must be distinct so as not to confuse them (the presence of a single dose system is useful in solving this problem.
· Inventory: Providing the appropriate inventory in quantity and quality.
· Environmental factors: Having a system designed to administer medication contributes to reducing errors, for example, “good lighting - distance from noise and interruptions .”
Giving the patient appropriate instructions regarding treatment
Understanding and adhering to hospital policy:
· Medications are substances whose misuse may pose risks to patients.
· There is a group of medications that have been agreed upon as high-risk medications.
· These medications are not placed in regular nursing departments.
· When used, a double review is done before it is given.
Fourth criterion
· Verifying the operation - the correct procedure - the correct patient.”
The problems of the wrong patient - the wrong procedure and the destination of the operation occur as a result of:
· Ineffective or incomplete communications between Health team members.
· Not involving the patient.
· Lack of policy.
· Failure to evaluate the patient.
· Not reviewing the patient's file.
Understanding and adhering to hospital policy:
· The policy is consistent with international standards to prevent an error on the part of the operation, procedure, or patient, as follows
· Determine the location of the operation
· The mark is placed before the patient is anesthetized.
· The mark is visible throughout the procedure
· Maryam's name in triple and the medical number
· The process is its destination
· Signatures and dates completed
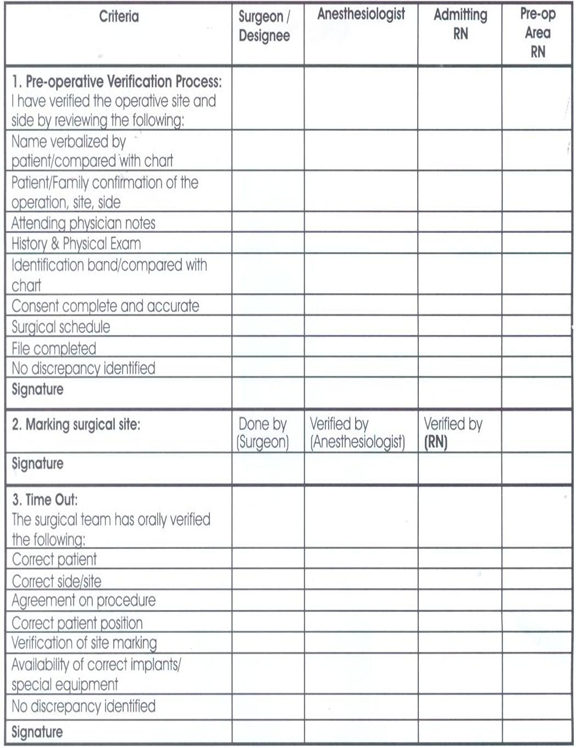
Verification process before the operation:
· Verify (the procedure provider - the patient - the name of the operation...).
· Verification is carried out by the floor nurse - the surgeon - the recovery nurse - the anesthesiologist separately.
· Verification is recorded in the special form and signature.
· Marked by the doctor or his assistant.
· Ensure availability of supplies.
· The surgeon must confirm with the operating nurse that...
· Supplies - Safety of used equipment - Providing machines
· Final verification Time Out: It takes place immediately before the start of the procedure. - It depends on team work and effective communication.
· The team consists of (the surgeon - the anesthesiologist - the nurse), and its purpose is to make sure that the correct procedure is performed on the correct patient in the correct direction .
Fifth standard:
Reducing the risk of infection in hospitals2
· The institution must establish a system that reduces the incidence of infection as a result of being in the hospital.
· The institution must adopt instructions and directives for hand hygiene.
A simple, low-cost process that reduces hospital infection rates. Hand washing remains the best way to reduce the transmission of infection
Hospitals' obligation to wash hands is not implemented effectively in all countries of the world, with variations.
Reasons for not adhering to hand cleaning:
◼️ The number of employees is less than the usual ratios.
◼️ Allergy to the materials used in cleaning.
◼️ Insufficient information available to workers about the importance or method of cleaning and individuals’ behaviors towards protecting patients
The following was observed regarding the commitment to clean hands:

◼️ Doctors are less interested in cleaning hands.
◼️ Nursing assistants are the least concerned about hand cleaning.
◼️ Males are less observant.
◼️ Intensive care workers are less committed.
◼️ Workers wearing gloves are less observant.
◼️ From the employees’ questions, the following was learned: “Their statements.”
◼️ The materials used cause allergies.
◼️ Lack of sufficient sinks for washing hands.
◼️ Unavailability of soap.
◼️ Always busy.
◼️ Patients' needs are most important.
◼️ We wear gloves.
◼️ There are no clear instructions.
◼️ The possibility of transmitting infection is small.
◼️ We don't remember.
◼️ We did not see female trainers or supervisors doing this.
Reducing the risk of infection in hospitals
What lives on the skin of the hands?
Colonizing microbes : They live continuously on the skin and are not usually affected by regular washing, but they are usually removed when washing with disinfectants.
Temporary microbes : They stick to hands when dealing with patients, contaminated tools and devices, or the surrounding environment. They are often responsible for transmitting infections in hospitals and are usually removed by routine hand washing .
Ways to take care of hand hygiene
Routine hand washing with soap and water.
Removing dirt - any organic materials - getting rid of temporary microbes.
Hands should be washed before and after:
- Performing any interventional procedure with the patient.
- Dealing with any wounds.
- Direct interaction with the patient - routine hand washing with soap and water.
- Removing dirt - any organic materials - getting rid of temporary microbes.
- Hands must be washed before: - Serving any meal - Leaving work - Caring for patients with weak immune systems.
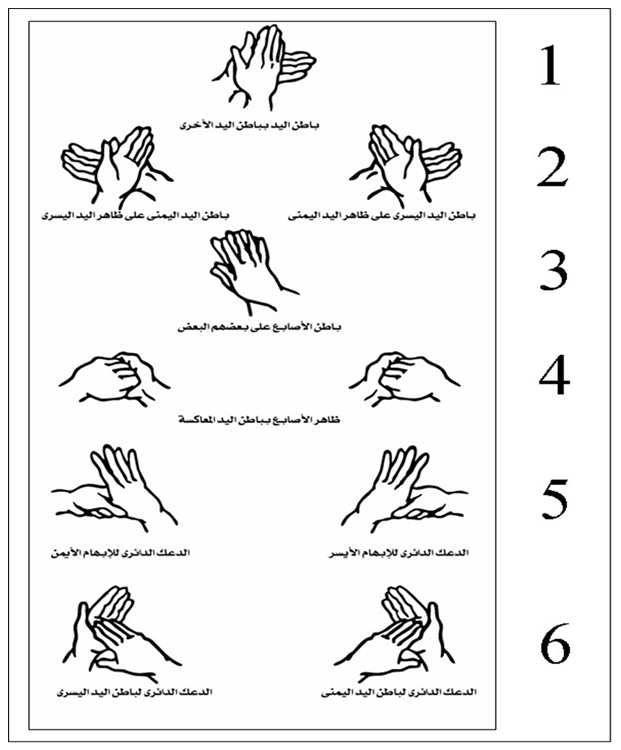
How to wash hands?
- Remove any jewelry and open the faucet with your elbow or hand.
- Wet hands with water, apply soap and distribute it on both hands.
Follow the picture instructions. Rinse hands. Dry hands well with a single-use towel. Close the tap with the same towel.
Sixth standard : Reducing the risk of falling.
A fall is a sudden and unexpected downward fall that may or may not result in injury.
How can patients who are at risk of falling be identified ?
· Evaluation is a process carried out by the nurse to collect data that helps identify the patient's problems.
· Evaluation is a procedure that involves several aspects, one of which is assessing the possibility of falling.
· The purpose is to identify patients at risk of falling so that the necessary precautions can be taken.
· The policy stipulates that all patients (departments - clinics) are evaluated for the possibility of falling.
· You will use an evaluation form within an hour for department patients and within 10 minutes for clinic patients.
· The assessment is repeated once every 24 hours. Those with scores of 0: 44 are classified from simple to moderate, and the following precautions are applied to them:
· Familiarizing the patient with his surroundings - the suitability of what he wears on his feet - the bed is placed in a low position.
· Install everything that is moving - good lighting - the patient’s personal needs are at his fingertips.
· The nurse call machine and telephone are working and in proper condition - the room is tidy and the floors are dry.
Know the patient:
· How to call the nurse when needed - Inform the nurse when you feel “dizziness - fainting...”.
· Use any aids used.
Those who obtained 45 or more must follow the following:
· Familiarize the patient with his surroundings several times.
· The nurse is there to help every time the patient is moved.
· The patient's room is close to the nursing station.
· The bed is in the low position and good lighting stabilizes everything that is moving.
· The patient's needs are at his fingertips.
· The nurse call machine and telephone are working and within his reach.
· The room is tidy, the floors are dry, and there are no obstacles in the patient’s path.
· The patient should not be left alone on a commode or wheelchair.
· What is worn on the foot to prevent slipping?
· The patient is asked every two hours during the day about his requests.
· He is followed quietly while working.
· Verbal mention is made of the possibility of falls among nurses when shifts are changed.
· This is written in the nursing notes.
· The importance of these precautions is discussed with the patient's family.
· The patient is asked every two hours during the day about his requests.
· He is followed quietly while working.
· Verbal mention is made of the possibility of falls among nurses when shifts are changed.
· This is written in the nursing notes.
· The importance of these precautions is discussed with the patient's family.
Seventh standard: Preventing disconnection or misconnection of catheters or tubes
v All connections are connected to the patient in the correct place.
v The name of the connection or catheter and the date of installation are written on it.
v The leads, catheters, and insertion site are taken care of for signs of infection and other signs.
The responsible nurse places an adhesive tape on which is written:
· Date of insertion of the catheter or tube.
· Type of catheter or tube.
· Size of catheter or tube.
· The person who installs the catheter or tube .
· And evaluating the placement and connection of the catheter or tube according to its type and the purpose of its installation or at the beginning of work shifts and during the delivery and receipt process .
Eighth standard: Preventing bed sores
· Bedsores are one of the nursing problems that may occur to patients when they are not taken care of.
· When the patient receives a new admission at the time of admission to the department and has bed sores, a declaration is written and signed by the patient or his companion stating that the patient has bed sores and of what degree they are.
· The nurse responsible for the patient examines the patient at risk of developing bed sores and determines his degree of exposure to bed sores. The treating physician and the responsible nurse
determine the degree of the pressure ulcer in order to know the medical care plan required for the patient. The doctor records the result of the evaluation in the patient’s medical record.
The patient exposed to bed sores is evaluated as follows
First degree: Redness in the area prone to ulcers compared to normal skin color. Coverarea.
Second degree : loss of the surface layer of the skin and the presence of a scarlet-red ulcer with the presence of white or yellow fluid, sometimescovering/protecting the skin/moisturizing and healingthe.
Third degree: The presence of a deep ulcer that includes the superficial layer of the skin and what lies beneath it / there is white, gray or yellow fluid / there is an edge to the ulcer / there is a purulent discharge. Covering the skin/protecting it/moisturizing and healing ulcers/removing dead tissue/cleaning and treating infections/aiding healing.
Fourth degree : The presence of a deep ulcer that reaches from the surface layer of the skin to the muscles and bones. There is a foul odor. There is a brown or black secretion. There is a purulent secretion. Covering the skin / protecting it / moisturizing and healing ulcers / removing dead tissue / cleaning and treating infections / helping healing / filling the gap.
Precautions to be taken to prevent bed sores :
◼️ If the patient is bedridden, he must use an air-filled mattress (air mattress).
◼️ Use pillows between the joints (knees, elbows).
◼️ Use soft, clean and dry furniture.
◼️ Avoid forming folds in the bedding under the patient.
◼️ Monitor the skin constantly (dryness, wetness, redness).
◼️ Dry the body well after washing.
◼️ Eat balanced food.
◼️ Consult a physical therapist regarding appropriate exercises to improve blood circulation.
Ninth standard: Risk management and patient safety:
Risk management is the other side of patient safety and security. The risks that the patient may be exposed to in the hospital are identified, an analysis is made of them, and a method is developed for how to deal with them, solve them, and prevent them from occurring again.
· There are risks that come from people.
· Risks resulting from interventions to which patients are exposed.
· Risks from hospital infrastructure.
· Risks arising from the wrong work system.
Tenth Standard: Delivery and Receipt Policy:
The Purpose:
Communicating important information about patient care from one doctor to another, from one nurse to another, or from one person to another during the patient’s medical service shift.
Politics:
The commitment of the medical service providers during the work shift to provide and exchange general information about the patient while providing medical care to him. The head of the department develops a handover and receipt form that contains the important information that is exchanged between the medical service providers in his department. The medical service providers deliver and exchange medical information among themselves. During the work shift, according to the relevant guides and forms, information is exchanged between service providers during the exchange of work sessions, with sufficient time to discuss information about the patient and provide answers to inquiries about the care or service required to be provided to the patient. The head of the department ensures the continuous implementation of the handover and receipt process in the event of a transfer. The Patient Medical service providers exchange important information about the patient and provide answers to inquiries about the patient’s condition during the handover and handover process. The information that must be conveyed orally or through handover and handover forms is: the patient’s name, age, date of birth and address Diagnosis History Patients Allergies Medications/Food/Liquids Tests/ Tests, previous and planned operations, the patient’s health care plan within 24 hours, tests and analyzes required to be performed, procedures required before the patient is discharged.
Standard Eleven: Isolation and restriction policy
· The Patient Care Law guarantees the patient his right to enjoy his freedom and not be restricted or isolated in accordance with Article (36) of the law unless the emergency situation requires it. Isolation or restriction is an exceptional situation that the treatment team does not resort to as part of the treatment plan because the principle is to avoid them and use them after Exhausting the means that least restrict the patient's freedom.
· The patient's emergency situation is represented by the emergence of aggressive behavior or disturbed behavior that threatens his safety or the safety of others around him and constitutes an imminent danger that cannot be controlled or contained by means that are less restrictive of his freedom (such as reassuring the patient, using positive reinforcement, or modifying the environment surrounding him).
· Isolation and restriction procedures shall not be applied except by direct order from the responsible physician or his representative within the facility who has experience in applying these procedures.
· The therapeutic team performing the isolation or restraint must be professionally trained in both procedures and possess the skills that qualify it to carry out them, taking into account the application of internationally approved standards.
· Isolation or restriction procedures must be carried out according to methods that are psychologically and physically safe and preserve the patient’s dignity.
· Isolation or restriction measures must not be a means of coercion, discipline, comfort or retaliation by the treatment team.
· Isolation or restriction procedures shall be carried out for a specific time and must be terminated immediately upon the expiration of the reasons that necessitated their application, provided that the period of isolation or restriction for adults shall not exceed 8 continuous hours in accordance with the provisions of Article (36) of the executive regulations of the law, subject to renewal, but only after another debate and a new examination of the patient. By the responsible physician or his representative. Renewal requires the continuation of the emergency situation, and it is preferable that the time specified for the isolation or restriction procedure be in accordance with international standards as follows: -
o 4 hours for adults (18 years or older)
o 2 hours for teenagers (9-17 years old)
o One hour for children under 9 years old
· A patient subject to restraint or isolation reserves the right to see an official of the Patient Rights Committee and also has the right to file a complaint.
Isolation :is detaining the patient against his will in a room or area designated for that purpose, isolated from others, so that he cannot leave it, provided that the place conforms to all internationally approved specifications for isolation rooms.
Restriction :It is the restriction of the patient’s movement and its types:
Manual restraint: - Manually or physically, the patient is contained with the least amount of force by immobilizing his arms and legs, avoiding pressure on his back and neck, and keeping his position lying on his back as much as possible.
Mechanical restraint: What is meant is the use of tools or devices to limit the patient’s movement so that they are close to his body to the extent that he cannot easily escape from them. It also allows him little freedom of movement. It is safe and provides the patient with physical and psychological protection. It keeps the patient from falling. It is easy to adjust and does not waste dignity. For the patient, it does not require surgical intervention to install it. It allows for quick termination when an emergency occurs in the patient’s surroundings.
· When restraining, one person is required on each limb and another for the patient's head. The patient is placed lying on his back in the bed, and each ankle and wrist are tied so that he is tied to the bed from four sides. Soft restraints are used, such as gauze, leather restraints, or medical belts, according to the desired degree of fixation and the patient's condition, and are not applied. Restraints on the chest, neck and head.
To apply isolation or restriction measures, the following steps must be followed:
· Observation of the patient by the treatment team present with him in terms of behavior and actions and quickly predicting the presence of imminent danger as a result of his behavior.
· The treatment team (often the department's nursing staff) monitors any aggressive behavior in the patient or severe agitation that threatens his safety or the safety of others around him and evaluates it professionally, not personally, towards the patient.
· Trying to use the means that are least restrictive of the patient’s freedom, and after exhausting them and not being able to control the emergency situation, the treatment team resorts to containing the patient and trying to control his movement with physical restraint only. It is not permissible to isolate the patient or restrain him chemically or mechanically except by direct order from the responsible physician or his representative. .
· Fill out the paragraph related to the nursing staff member’s report on the emergency case in the isolation and restraint form
· Call the responsible doctor or his representative immediately to discuss the case and do the following:
o Clinical examination of the patient (psychologically and physically)
o Evaluate the extent of the risk and whether it requires the application of isolation or restraint measures, and attempts to control it by means that least restrict the patient’s freedom.
o Informing the patient of the reasons that necessitated isolation or restriction measures, the danger of his behavior to himself and others, and quickly ending the procedure if the reasons necessitating it do not exist.
· The responsible physician or his representative must complete the form for isolation and restraint, which includes:
o Clinical examination of the psychological and physical patient
o Risk aspects and severity
o Less restrictive means that have been exhausted
o The specified period of isolation or restriction
o The type of procedure that will be decided for the patient
o Description of the prescribed method of isolation or restraint, for example (the place of isolation is the patient’s room or another room - the mechanical restraint, the nature of the tools used in the procedure and how they are used and distributed among the parts of the body)
o Determine the start and end times of the procedure in isolation or restraint
o Pointing out the necessity of observing critically ill patients such that their condition requires special care, for example: patients with respiratory diseases, heart diseases, and patients with obesity and overweight.
o The responsible physician or his representative must state his name, signature, and the date of the procedure
o The procedure is performed under the direct supervision of the responsible or on-call physician and in the presence of one of them
o Identifying the cases and circumstances that require the treatment team to complete the procedure
o The responsible physician or his representative must review the patient’s treatment plan and update it according to the patient’s clinical condition and the circumstances surrounding him to avoid a recurrence of the emergency.
· A member of the therapeutic team is assigned to observe the patient face to face around the clock throughout the specified period of isolation or restriction, and to follow up on him every 15 minutes and record the following:
o Injuries that the patient may have suffered during the procedure
o Vital signs, respiratory rate, nutrition, skin color, behavior, and general condition
o Condition of blood circulation in the places of restriction (pulse, skin color)
o Movement rate, provided that restrictions are lifted every two hours for 10 minutes
o Provide him with fluids for two hours and record his intake
o The patient is given two hours of time to excrete (urine, stool) when needed
o It allows the patient to sleep and provides him with protection and comfort during sleep
o Ensure that restrictions are placed in their correct places and amend them when necessary
o Protecting the patient from others harming him (verbal and physical) during the procedure
o Observing the patient's ability to understand the procedure, his ability to adapt to it, and the form of his behavioral response
o The name of the nursing staff member performing the procedure and observation must be recorded on the isolation and restraint form
· The hospital is committed to creating a special record of isolation and restriction procedures, which records:
o Patient's name, registration number, admission date
o The type of procedure, its date, and its duration
o Name of the responsible physician and nursing staff member performing the procedure and observation
· The record is presented to the medical director daily, and the hospital administration is notified of this action immediately after it is taken during working hours or immediately the next morning when it is implemented in the shift.
Reasons for ending isolation or restriction measures:
· The signs of danger that necessitated applying the procedure have disappeared and the emergency situation has disappeared
· The success of one of the least restrictive means of the patient's freedom to control and modify the patient's behavior
· The appearance of signs of deterioration in the patient's organic condition requires terminating the procedure
· The occurrence of an emergency in the vicinity of the procedure that prevents its completion, such as a fire.
- Records and reports
The work of the nursing staff includes its various types, from the chief nurse to the inspectors- Supervisors and nurses write many reports and record health and nursing data.
The process of measuring performance and planning health nursing services depends on the accuracy of registration and the efficiency of records and reports. Therefore, attention must be paid to records and reports so that the information is correct, complete, accurate, recorded in a clear manner, and kept in a safe place so that it is not damaged or lost.
The importance of records and reports:
Records and reports have many important benefits that can be summarized as follows:
1- A record of the unit’s work and the nurse’s work in terms of quantity and type so that it can be referred to when necessary.
2- One of the means used to evaluate the performance of the unit and workers.
3- Means of communication between the employee and the authorities.
4- A tool for guidance when planning health and nursing services.
5- A tool for guidance when organizing educational programs and training courses.
6- A way to learn about the situation in society, common problems and diseases, and ways to treat them.
7- A tool for conducting comparative research in the fields of health and nursing.
8- A document that can be relied upon in legal problems to protect health workers and institutions .
Characteristics of good recording and reporting:
1- Accuracy, clarity and honesty in recording.
2- The data must be complete, correct, neatly arranged and objective.
3- Accuracy of timing when reporting certain important information, incidents, or disasters that cannot be postponed, as reporting must occur immediately and at the specified time.
4- The report must end with the signature of the informant or writer, the date, and sometimes also the time.
Reports:
A report is an oral or written message, the purpose of which is to convey information about a specific topic or incident for recording, reporting, or to take a specific action. Usually, reports are submitted from the subordinate to the superior on a regular basis and at specific times, with the exception of accidents and disasters, which are reported immediately upon their occurrence.
A good report is one that conveys information in a clear and precise manner, using simple sentences and without repetition- Use clear words that do not contain ambiguity or carry more than one meaning -And avoid using the building for the unknown -Choose the appropriate words that clarify the purpose -Ensure accuracy in writing, taking into account that there is sufficient time for drafting and review before signing, and a copy of the report must be kept for reference when necessary.
The report usually consists of the following parts:
1- Name of the person or entity to whom the report is sent.
2- Report Title- It must be brief, clear, and indicative of the subject of the report.
3- A simplified summary of the topic.
4- The introduction includes a quick presentation of the history of the topic, its development, and the special circumstances surrounding it in terms of time, place, and people
5- Body of the report- Or the main part of the report, which includes a complete presentation of the topic based on observations, interviews, and documents.
6- The conclusion reached by the report writer and his personal opinion for treatment or solutions.
7- Conclusion and recommendations.
8- Signature and date.
There are many types of reports:
Including printed and standardized forms in all hospitals and units, such as statistical reports, reports attached to samples for laboratories, or a request to perform x-rays. ... etc.
There are also verbal reports, such as what the nurse informs her colleague in the next shift, such as the condition of a particular patient or a special treatment that is required to be performed. It is preferable to record this information in a written report as well for reference when necessary.
Methods of communication from the boss to the subordinate (from top to bottom) are in the form of administrative orders or instructions -Work guide -Bulletin board periodicals -Sometimes they are in the form of verbal instructions.
Most written communications that travel down from management to workers are issued in the form of administrative orders, work manuals, and bulletin board periodicals.
As for written data and information that come from workers to the top, they may include statistical data and information about the quantity and type of services, and written reports from subordinates to superiors may affect service planning and decision-making to solve problems, resulting in the achievement of goals. Good management gives instructions and directions to workers about the quality of data. The statistical information that must be included in the report for each nursing department or unit.
As for the reports prepared by supervisors or head nurses and inspectors, they are usually related to solving problems, what has been done and what should be done, as well as an evaluation of current production and quality of care, along with presenting suggestions to solve problems that are outside their control and authority. Written reports can be kept as documents and a source that can be referred to if they contain Provides correct, accurate and real information.
Reports related to nursing services management:
1 - Report of receipt and delivery of the shift:
Necessary as a means of communication to transfer and follow up information from one group of nurses to another group during the daily 24-hour work. These written reports provide the nurse with notes about the patients and what happened to them during the period preceding their work. The importance of this report is that a large number of nurses and members of the health team meet with The head nurse is required to provide the necessary data before writing the report, raise any questions, and reach clarifications and solutions to problems. The shift report makes the nurse aware of what happened.
2- Daily report:
This report is written by the hospital’s head nurse to the director to inform him about:
- General condition of the hospital.
- Statistics of patients who had changes or complications.
- Cases of patients who have undergone changes or complications.
- Patient cases that follow specific treatment or research.
- Entry, exit, transfer and death cases.
- critical cases .
- The plan to be followed in the event of an emergency.
- All cases with high fever, especially after birth.
- Complaints from patients or service users.
- There are many forms of this type of daily general report.
3- Patient census report:
It is the official number of patients in the inpatient department or in hospital departments at a specific time, usually at midnight. The overnight nurse is responsible for writing this report, and its purpose is to know the number of patients in the inpatient department at any time, the bed occupancy rate, and the number of empty beds.
4 - Reports on work problems and the extent of progress in following the proposed solutions:
Writing reports on work problems and giving recommendations for solving them is an effective tool for obtaining facts and helping to direct discussion of a particular problem in meetings, as well as providing guidance for the follow-up system.
These reports also help other nurses, all members of the health team, and superiors know the real reasons behind these problems, so that they can confront similar problems that occur in the future and when evaluating progress in solving these problems and achieving the desired goals of work.
The following must be followed when writing reports on work problems:
1- Definition of the problem and its size.
2- Giving an accurate statement of the errors and what needs to be fixed.
3- Analyze the reasons that led to these errors.
4- Remember the roots of the problem as the report writer sees it.
5- Proposed solutions to eliminate the causes of the problem, along with clarifying the people who will implement the solutions.
5- Reports on accidents and emergency situations:
The responsibilities of the nursing staff are to maintain the safety and well-being of patients and users of health services in hospitals and health units.
They are responsible for implementing and following up on the treatment and nursing plans for these patients, as well as for avoiding accidents and dangers that may occur in hospitals and health units. In order to provide insight and determine the duties of nursing staff members in the event of disasters or an emergency, they must be introduced to the hospital or unit system and how to inform their superiors. Work when internal disasters occur, as well as how to carry out their duties in response to them.
Therefore, one of the most important duties of the nursing services department in hospitals and health units is to follow a special system for reporting the occurrence of such errors and accidents as soon as they occur, and to alert and train nurses when they take up work on the necessity of reporting these errors and accidents to those responsible. One of the most effective methods of reporting is writing reports on accidents and emergencies.
Reports of medication administration errors:
Such errors may occur from members of bodies that deal with issuing, preserving, or administering treatment to the patient, such as nursing staff, pharmacists, and technicians. This may indicate that they did not follow the necessary procedures of the hospital in giving and dispensing treatment. This may also be an indication that the doctor’s orders are necessary. It must be written accurately and clearly, and the pharmacy instructions written on the packaging must also be written accurately and clearly.
Analysis of reports on accidents that occur to patients during their stay in the hospital or their visit to health units shows a lack of accuracy on the part of those responsible for caring for the patients. For example, negligence in not following the instructions issued by the head nurse regarding the operating room, which must be followed by the nursing staff and doctors, such as counting the technician’s towels before closing the wound. During the operation, the shortage of these pads is discovered before the opportunity is too late, so that the hospital bears this responsibility alongside the doctors and nursing staff.
Likewise, accidents may occur for workers due to failure to follow the appropriate method and methods at work. For example, when linens are not checked before putting them in their container to be sent to the laundry, the laundry workers may be exposed to injury from quickly leaving scalpels or sharp tools in them.
For each of these examples, it appears that nursing staff members have an important effective role in preventing accidents and mistakes that may result to patients and workers that may happen to the patient while he is in the hospital. Therefore, reports on the patient’s physical and mental condition must be recorded in the patient’s file and notified to the head nurse and the doctor. Whoever is responsible at the time, such as the appearance of bed sores or lice infestation, as well as an unwanted reaction to a treatment such as the occurrence of chills (shivers) when giving intravenous solutions or injections, must be recorded and reported to the specialist as incidents and recorded in writing in a report.
The report of emergency incidents and treatment errors includes the following:
Patient's name and diagnosis.
Date of entry, frequency, or visit.
Time to notice and report the situation.
What was done to prevent the condition from occurring?
The circumstances of the situation, its dimensions, and the unusual factors that affected the environment at the time the situation occurred.
Steps taken to correct the situation and remedy the error.
Date, signature of individuals writing the report.
Suggestions from the head nurse to prevent such an error from occurring and are sent to the director of the hospital or health unit .
6- Reports on patient complaints:
The patient's complaint must be reported immediately to the head nurse, and it is important for both the nursing team leader and its members to become aware of the patients' complaint and their relatives from the beginning of the complaint so that it does not escalate and so that it facilitates the study and analysis of nursing plans to find appropriate solutions at the right time.
It is possible that complaints submitted by patients and their relatives regarding the quality of services provided constitute a kind of effective participation in directing these services in the interest of patients, workers, and the institution alike, by involving the patient in implementing the plan drawn up to care for him. Therefore, nursing staff members must consider the complaint objectively. The patient is assisted in accepting the necessary adaptation while he stays in the hospital, implementing his treatment, and accepting health instructions.
Such a report includes the following:
· The content of the complaint and its justifications as stated by the patient.
· Actions taken to resolve the complaint.
· The result .
· Date and signature .
7- Administrative reports:
Sometimes the executive authority and directors of hospitals and health units request writing and submitting monthly, quarterly, or annual reports from each department or unit of the institution or hospital. The Nursing Services Department may request written and periodic reports from the heads of nurses and nursing units in the hospital. Likewise, nursing inspectors often request monthly reports from Head nurses of health units.
Such a report includes the following:
· A brief account of the unit’s activities, the type of nursing staff, the number of working hours and shifts, and statistics on births, admissions, discharges, deaths, and home visits.
· Current capabilities of machines, tools and maintenance status.
· Problems affecting nursing care in terms of manpower, environment, machines and tools.
A narration of the reasons for bringing about a change in the work pattern in terms of labor or resources and the result of this change, giving evidence and indicators that prove these changes and their results.
These reports must be taken seriously by superiors and their results must be followed up until the changes required to raise the level of services in health units are made. If they are not taken seriously, these reports are considered a waste of time and energy and become unproductive. …
Records:
The Definition :
Records are an administrative tool used to preserve and arrange information and prevent its repetition. They contribute to achieving the goals of administration, the educational process, and conducting scientific research.
The following are the different types of records used in hospitals and nursing units:
1- Patient file:
It is the document that indicates the quality of health care given to patients or beneficiaries of health services. It includes information pertaining to the patient since his admission to the hospital or his first visit to the health unit, as well as his laboratory tests, observations, details of therapeutic procedures, as well as the patient’s reaction to the treatment and services provided to him.
* It also contains records of consultations for treatment and surgeries.
* It also has separate papers to record treatment and medications.
They are not only records to collect information about the patient, but they are also considered a legal document used when necessary in judicial cases, and therefore the data contained in the patient’s file has a privacy character.
There are many efforts being made to raise the level of efficiency of using records as an administrative tool at all levels of health services.
The patient's record (file) is used for the following purposes:
· Helping to reach diagnosis and treatment.
· Recording the services provided to the patient.
· Contributing to education and conducting research after the patient’s approval.
· It is used as an important legal document in cases brought before the judiciary.
· It is used in quantitative and qualitative analysis when evaluating services
The nurse's responsibility regarding patient files:
Organizing and arranging the records of new patients and patients, provided that these files include the following:
· Complete personal data for patients and visitors.
· Forms for vital signs and nurse notes.
· Laboratory forms, x-rays, and other records for specialized departments
· Treatment papers.
Responsibility of the unit head nurse towards keeping patient records:
· Records must be kept in a safe place away from tampering and loss.
· Do not give records to others unless the patient is referred for study or to the treating physician.
· Do not delete any paper from the patient’s or patient’s file for any reason.
· No one, including relatives, friends or families of patients, is allowed to read the records except with written permission from the director of the hospital or unit.
· Providing guidance and training to new nurses on how to take complete and correct notes.
· When the patient is discharged, you must ensure that the record is organized, correct, and complete before sending it to the office responsible for its preservation.
· Patient records and reports must contain the patient’s progress from his admission until his exit from the unit, and the details must be sufficient so that it is easy to use in following up on the patient’s condition whenever necessary, as well as when conducting scientific research .
2- Records for recording the nurse’s notes:
This includes recording accurate observations about the patients’ condition and the nursing care given to them. It also includes special information related to medications, treatment, food, and health instructions, as well as recording notes about the patient’s physical and psychological condition, the patient’s reaction to treatment, the extent of his adaptation to the disease, and any change that may occur in his condition.
The purpose of this record:
· There should be a unified record agreed upon by all employees in one hospital for writing notes by nurses to facilitate the transfer of responsibility from one nurse to another during different working hours.
· Facilitating the rapid review of the patient's condition and the performance of nursing care.
· Emphasize the importance of recording the nurse's notes.
3- Records of distribution of duties to members of the nursing team:
· It includes the names of the nursing staff members working in the unit and the names of the patients assigned to their care, as well as the special duties assigned to each of them. There must be a unified form that is filled out daily by the head of the unit’s nursing staff, and this record must be placed in a clear and known place for everyone.
The record of assignment distribution includes the following:
· Name of the nurse in charge.
· Patient name .
· Diagnosis.
· Needed nursing care or special treatment and research.
· The type of duties the nurse is responsible for, such as assisting the doctor in examining or giving treatment to patients.
· As well as special duties such as preparing to give injections or preparing the dressing cart for wounds.
The purpose of this record:
· Informing the nursing team members working in nursing units in hospitals and health units in writing about their daily responsibilities.
· Determine nursing responsibility for each patient.
· A basis for evaluating nursing care given to patients.
4- Shift tables:-
· It is a record that is prepared weekly and daily and specifies the plan drawn up to cover the nursing and health unit with nursing staff over a 24-hour period and includes the following:
· Names of the unit's nursing staff.
· The different levels of nursing staff members are in groups over the course of a week with a detailed 24-hour schedule on the number of shifts.
· Name of the head nurse in each shift.
· Rest days, sick leave, excuses and absences.
· Meeting times, rest hours, and lunch.
The purpose of this record:
· It shows the units' coverage of the nursing workforce and the extent of its adequacy.
· The presence and absence of nursing staff in the unit is recorded daily.
· It provides information about all nursing services in relation to the numbers and levels of the workforce.
· It also shows the number of working hours for each nurse.
5- Custody inventory records:
· Labeled records for all appliances, furniture, tools, and machines, specifying the quantity, specifications, and condition of each.
The purpose of this record:
· Providing the head nurse with information about tools that are missing, broken, or need to be repaired
· Return the surplus to its appropriate place, as well as the borrowed tools, before counting or inventorying the item.
6- Employee performance evaluation records:
These are records used to evaluate the performance of employees annually or every six months.
The Purpose :
· An objective basis on which employees are promoted and given rewards and incentives.
· An incentive for employees' professional advancement.
· It explains the reasons for poor performance and gives recommendations for good work.
7- Time tables:
· For routine and non-routine work.
The purpose :
· It shows the time when activities occur, which are daily, weekly and monthly.
· Daily schedules show the times when the unit's routine activities occur.
Monthly time sheets such as when monthly reports and orders are submitted.
1.
Supervision
notebook.
Patient entry and exit record book.
Department delivery and receipt book.
Nursing records book.
Emergency vehicle delivery and delivery book.
Delivery and delivery book for sterilization.
Patient treatment notebook.
Medical report book.
Medication dispensing book from the pharmacy.
X-ray order book.
Notebook of unexpected events.
Furniture notebook.
Maintenance book.
Malfunction reporting book.
Daily cash register.118