First Part
- International standards and goals for patient safety and security
The Definition
A common goal that requires the process of coordinating the efforts of the health staff with the patient to protect him from injuries. A process provided by the institution to make the health care provided more advanced, safe and secure. The process of preventing unexpected patient injuries.
Principles and standards of patient safety and security:
Risk assessment: environment - patient .
Identifying risks: - developing a plan to protect the patient - how to act when an error occurs - recording and analyzing the incident -
Determine the cause - develop solutions to reduce the reoccurrence.
Who is responsible for the patient's security and safety?
Patient safety and security standards are the right of every patient and the responsibility of all employees of the medical institution.
No employee is excluded, regardless of their administrative responsibilities:
Senior management, department managers and employees
Patient safety and security standards:
1. Introducing the patient in the correct way.
2. Improving good and effective means of communication.
3. Safety of using high-risk medications.
4. Ensuring the operation, the correct procedure, and the correct patient.
5. Reducing the risk of infection by washing hands.
6. Reducing patient falls to prevent injuries.
7. Preventing disconnection or misconnection of catheters or tubes.
8. Preventing bed sores.
1- Risk management and patient safety.
10. Delivery and pickup policy.
11Isolation and restriction policy.
First criterion:
1. Introducing the patient in the correct way:
Failure to introduce the patient in the correct manner leads to:
· Giving the medicine to another patient.
· Performing a procedure on another patient.
· Delaying giving treatment or performing a procedure.
· Giving an incorrect diagnosis.
· Connecting a wrong patient to operations .
· Cancel an operation.
Why does an error occur in the definition?
· Multiple interventions.
· Multiple places to provide the service.
· Multiple individuals dealing.
· Some patients are unable to identify themselves.
· Lack of a clear definition system.
How do we avoid identification errors?
· Don't worry - take the time.
· Do not depend entirely on the patient.
· Make sure the information, stickers, and identification bracelet are correct.
Do the following:
· Introduce the patient in the correct manner upon entry.
· Make sure the patient's name is as it appears on the ID card.
· Make sure the identification data is correct before putting it on.
· Put on a new bracelet if you lose the old one.
· Ensure that the patient complies with the required procedure.
· Ensure that the patient is properly matched before transferring him.
· Apply a sample identification label immediately after taking the sample and before leaving the patient.
Do not do the following:
· Do not dictate to the patient His name, but let him tell you his name.
· Do not take any sample before matching the patient with the data on the sample request form.
· Do not label the sample identification on the container before taking the sample.
· Do not complete the work of the procedure remotely.
Understand and adhere to hospital policy:
· The hospital’s commitment to international goals for patient safety and security :
· Patients are identified by their admission site.
· The hospital’s commitment to at least two definitions:
· Patient's name is quaternary.
· His medical code.
Both definitions are verified each time when:
· giving medicine .
· Sample collection.
· Giving blood or its derivatives.
· Do any tests.
· Take any other action.
Second criterion:
Improving effective communication methods.
The means of communication that most lead to errors:
· Verbal orders.
· Telephone orders.
Receiving test results verbally or by telephone.
Verbal orders: administered face to face between the sender and the receiver .
Telephone orders: administered through the telephone between the sender and the receiver .
Responsibility of the recipient of the message or order:
· Writing the order or message while dictating orally or by telephone.
· Read the matter to the sender and wait for a response with a comment.
· If the matter is related to giving medicine, it must include the five basics.
· After reading the order, the receiver completes the order data by writing the date and time, the recipient’s name and position, the sender’s name and position, and then signing.
· In emergency situations, such as a “cardiac arrest,” it is sufficient to repeat the command to the sender and wait for a response with feedback.
Responsibility of the sender or giver of the order:
· Sign the order quickly.
· Spell the name of the medication if necessary.
· The numbers are dictated as they are pronounced, then each number is mentioned separately.
· Gives the command without using the abbreviation.
v Understanding and adhering to hospital policy:
· The hospital accepts verbal and telephone orders within very limited limits when it is impossible to write them by the person responsible for them and if delaying them may affect the patient.
· The sender and receiver must abide by their responsibility in this regard.
· The sender's signature on the given order shall be made no later than 24 hours.
Third criterion
Safety of using high-risk medications.
Definition of high-risk medications:
These are medications that, if used in an inaccurate and improper manner, may lead to serious injury or death to the patient.
The most important of these medications are:
· Insulin.
· Narcotic medications.
· Anticoagulants.
· Potassium chloride KCl And potassium phosphate.
· Sodium chloride solution more than 0.9.
Why do errors occur and suggestions for preventing them?
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
· Develop and disseminate a bilateral review policy |
· Lack of bilateral review policy |
Insulin |
|
· writing“Unit”instead of U |
· Use the letter U Expressed as the number of units |
|
|
· They are placed in different and labeled shelves |
· Place the insulin container near the heparin container |
|
|
· Use self-programming or dual-review pumps |
· Incorrect programming of the solution pump |
|
|
· Coordination between them |
· Do not link insulin administration with meals |
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
· Limiting their presence to their designated places |
· Put them in the regular departments with the stock of other medicines |
Drugs Morphine |
|
· Develop and disseminate a narcotic drug policy |
· Lack of policy and procedure for its use |
|
|
· Preparing printed medical orders explaining what is used in cases of mild to moderate pain · * It is necessary to have a doctor in case of severe pain |
· Using verbal or telephone orders |
|
|
· Use a pain assessment form |
· There is no way to evaluate pain |
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
· Not to be placed in regular nursing departments |
· Presence in regular nursing departments
|
Potassium chloride And Potassium phosphate |
|
· the chapter Among them in storage and preservation places |
· Mixing the two medications |
|
|
· Unify focus |
· Do not put a sticker Dosage and quantity after preparation |
Anticoagulants (heparin) |
|
· Use single dose containers |
· Use multi-dose containers |
|
|
· Separation of the two medications |
· Confusion between heparin and insulin |
|
|
· Relating doses to laboratory results |
· Determine doses without relying on laboratory results |
|
Error prevention proposals |
Reasons for the error to occur |
Medicine |
|
o Limiting his presence to care - operations - pharmacy |
o Its presence in regular nursing departments |
Sodium chloride at a concentration of more than 0.9% |
|
o Develop and disseminate a bilateral review policy |
o Lack of bilateral review policy |
o General instructions to reduce the risks of giving medications in general:

· Passing the “drug review” test is a condition for allowing treatment to be given.
· The presence of a pharmaceutical reference for some medications.
· Develop a bilateral review policy by two nurses and circulate it.
· Linking the administration of some medications to laboratory results.
· link Giving analgesics by assessing pain.
· Delete the presence of high-risk medications from the sections.
· Lack of medicines with similar packages and similar taste in one place.
· Place a clear label with the name in the place where each medication is kept and stored.
· Review the use of a two-way solution pump.
· After administering the treatment for the first time, the medication label is compared - according to the medical order - to the medication administration record sheet. When administration is repeated, the medication label is compared to the medication administration registration sheet.
· Identifying, recording, analyzing errors and finding out the reason is the path to improvement.
Keys that help avoid errors when giving treatment:
· Information about the patient.
· Information about the medicine.
· Effective Communication .
· Labeling of pharmaceutical packages: Medicines with similar packages or with a similar sound must be prepared when preparing their packages. Each package must be distinct so as not to confuse them (the presence of a single dose system is useful in solving this problem.
· Inventory: Providing the appropriate inventory in quantity and quality.
· Environmental factors: Having a system designed to administer medication contributes to reducing errors, for example, “good lighting - distance from noise and interruptions .”
Giving the patient appropriate instructions regarding treatment
Understanding and adhering to hospital policy:
· Medications are substances whose misuse may pose risks to patients.
· There is a group of medications that have been agreed upon as high-risk medications.
· These medications are not placed in regular nursing departments.
· When used, a double review is done before it is given.
Fourth criterion
· Verifying the operation - the correct procedure - the correct patient.”
The problems of the wrong patient - the wrong procedure and the destination of the operation occur as a result of:
· Ineffective or incomplete communications between Health team members.
· Not involving the patient.
· Lack of policy.
· Failure to evaluate the patient.
· Not reviewing the patient's file.
Understanding and adhering to hospital policy:
· The policy is consistent with international standards to prevent an error on the part of the operation, procedure, or patient, as follows
· Determine the location of the operation
· The mark is placed before the patient is anesthetized.
· The mark is visible throughout the procedure
· Maryam's name in triple and the medical number
· The process is its destination
· Signatures and dates completed
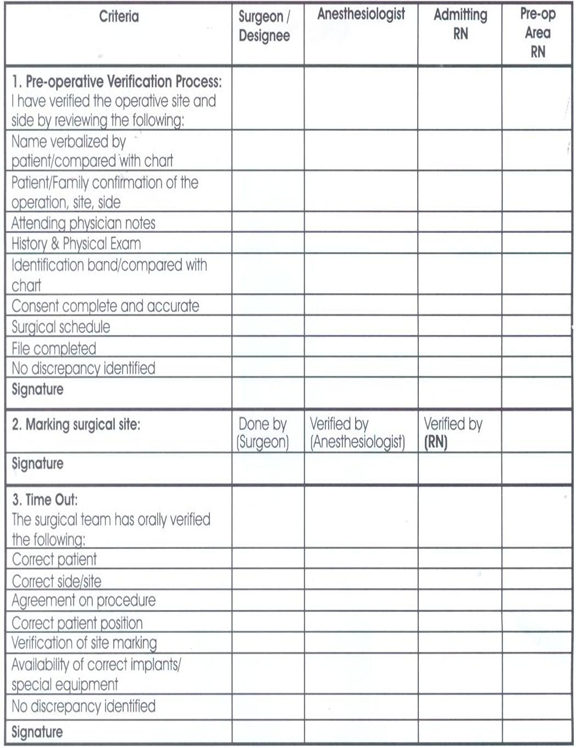
Verification process before the operation:
· Verify (the procedure provider - the patient - the name of the operation...).
· Verification is carried out by the floor nurse - the surgeon - the recovery nurse - the anesthesiologist separately.
· Verification is recorded in the special form and signature.
· Marked by the doctor or his assistant.
· Ensure availability of supplies.
· The surgeon must confirm with the operating nurse that...
· Supplies - Safety of used equipment - Providing machines
· Final verification Time Out: It takes place immediately before the start of the procedure. - It depends on team work and effective communication.
· The team consists of (the surgeon - the anesthesiologist - the nurse), and its purpose is to make sure that the correct procedure is performed on the correct patient in the correct direction .
Fifth standard:
Reducing the risk of infection in hospitals2
· The institution must establish a system that reduces the incidence of infection as a result of being in the hospital.
· The institution must adopt instructions and directives for hand hygiene.
A simple, low-cost process that reduces hospital infection rates. Hand washing remains the best way to reduce the transmission of infection
Hospitals' obligation to wash hands is not implemented effectively in all countries of the world, with variations.
Reasons for not adhering to hand cleaning:
◼️ The number of employees is less than the usual ratios.
◼️ Allergy to the materials used in cleaning.
◼️ Insufficient information available to workers about the importance or method of cleaning and individuals’ behaviors towards protecting patients
The following was observed regarding the commitment to clean hands:

◼️ Doctors are less interested in cleaning hands.
◼️ Nursing assistants are the least concerned about hand cleaning.
◼️ Males are less observant.
◼️ Intensive care workers are less committed.
◼️ Workers wearing gloves are less observant.
◼️ From the employees’ questions, the following was learned: “Their statements.”
◼️ The materials used cause allergies.
◼️ Lack of sufficient sinks for washing hands.
◼️ Unavailability of soap.
◼️ Always busy.
◼️ Patients' needs are most important.
◼️ We wear gloves.
◼️ There are no clear instructions.
◼️ The possibility of transmitting infection is small.
◼️ We don't remember.
◼️ We did not see female trainers or supervisors doing this.
Reducing the risk of infection in hospitals
What lives on the skin of the hands?
Colonizing microbes : They live continuously on the skin and are not usually affected by regular washing, but they are usually removed when washing with disinfectants.
Temporary microbes : They stick to hands when dealing with patients, contaminated tools and devices, or the surrounding environment. They are often responsible for transmitting infections in hospitals and are usually removed by routine hand washing .
Ways to take care of hand hygiene
Routine hand washing with soap and water.
Removing dirt - any organic materials - getting rid of temporary microbes.
Hands should be washed before and after:
- Performing any interventional procedure with the patient.
- Dealing with any wounds.
- Direct interaction with the patient - routine hand washing with soap and water.
- Removing dirt - any organic materials - getting rid of temporary microbes.
- Hands must be washed before: - Serving any meal - Leaving work - Caring for patients with weak immune systems.
How to wash hands?
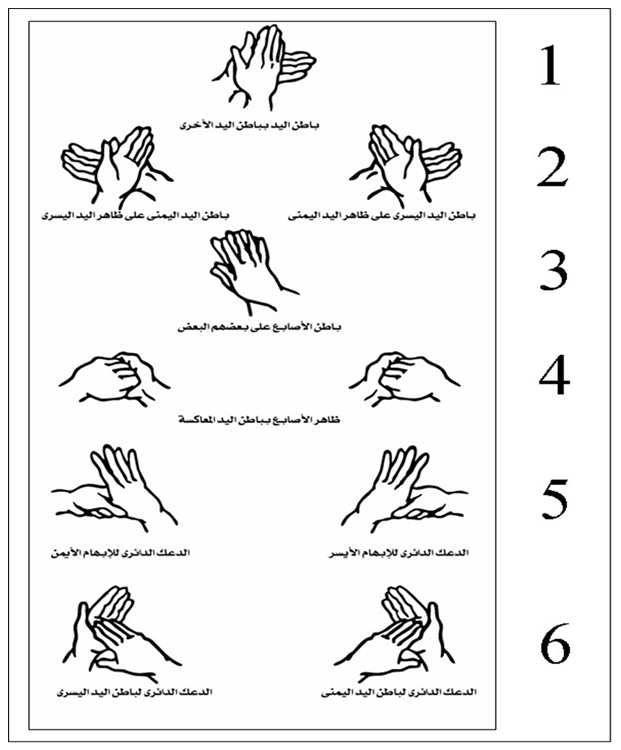
- Remove any jewelry and open the faucet with your elbow or hand.
- Wet hands with water, apply soap and distribute it on both hands.
Follow the picture instructions. Rinse hands. Dry hands well with a single-use towel. Close the tap with the same towel.
Sixth standard : Reducing the risk of falling.
A fall is a sudden and unexpected downward fall that may or may not result in injury.
How can patients who are at risk of falling be identified ?
· Evaluation is a process carried out by the nurse to collect data that helps identify the patient's problems.
· Evaluation is a procedure that involves several aspects, one of which is assessing the possibility of falling.
· The purpose is to identify patients at risk of falling so that the necessary precautions can be taken.
· The policy stipulates that all patients (departments - clinics) are evaluated for the possibility of falling.
· You will use an evaluation form within an hour for department patients and within 10 minutes for clinic patients.
· The assessment is repeated once every 24 hours. Those with scores of 0: 44 are classified from simple to moderate, and the following precautions are applied to them:
· Familiarizing the patient with his surroundings - the suitability of what he wears on his feet - the bed is placed in a low position.
· Install everything that is moving - good lighting - the patient’s personal needs are at his fingertips.
· The nurse call machine and telephone are working and in proper condition - the room is tidy and the floors are dry.
Know the patient:
· How to call the nurse when needed - Inform the nurse when you feel “dizziness - fainting...”.
· Use any aids used.
Those who obtained 45 or more must follow the following:
· Familiarize the patient with his surroundings several times.
· The nurse is there to help every time the patient is moved.
· The patient's room is close to the nursing station.
· The bed is in the low position and good lighting stabilizes everything that is moving.
· The patient's needs are at his fingertips.
· The nurse call machine and telephone are working and within his reach.
· The room is tidy, the floors are dry, and there are no obstacles in the patient’s path.
· The patient should not be left alone on a commode or wheelchair.
· What is worn on the foot to prevent slipping?
· The patient is asked every two hours during the day about his requests.
· He is followed quietly while working.
· Verbal mention is made of the possibility of falls among nurses when shifts are changed.
· This is written in the nursing notes.
· The importance of these precautions is discussed with the patient's family.
· The patient is asked every two hours during the day about his requests.
· He is followed quietly while working.
· Verbal mention is made of the possibility of falls among nurses when shifts are changed.
· This is written in the nursing notes.
· The importance of these precautions is discussed with the patient's family.
Seventh standard: Preventing disconnection or misconnection of catheters or tubes
v All connections are connected to the patient in the correct place.
v The name of the connection or catheter and the date of installation are written on it.
v The leads, catheters, and insertion site are taken care of for signs of infection and other signs.
The responsible nurse places an adhesive tape on which is written:
· Date of insertion of the catheter or tube.
· Type of catheter or tube.
· Size of catheter or tube.
· The person who installs the catheter or tube .
· And evaluating the placement and connection of the catheter or tube according to its type and the purpose of its installation or at the beginning of work shifts and during the delivery and receipt process .
Eighth standard: Preventing bed sores
· Bedsores are one of the nursing problems that may occur to patients when they are not taken care of.
· When the patient receives a new admission at the time of admission to the department and has bed sores, a declaration is written and signed by the patient or his companion stating that the patient has bed sores and of what degree they are.
· The nurse responsible for the patient examines the patient at risk of developing bed sores and determines his degree of exposure to bed sores. The treating physician and the responsible nurse
determine the degree of the pressure ulcer in order to know the medical care plan required for the patient. The doctor records the result of the evaluation in the patient’s medical record.
The patient exposed to bed sores is evaluated as follows
First degree: Redness in the area prone to ulcers compared to normal skin color. Coverarea.
Second degree : loss of the surface layer of the skin and the presence of a scarlet-red ulcer with the presence of white or yellow fluid, sometimescovering/protecting the skin/moisturizing and healingthe.
Third degree: The presence of a deep ulcer that includes the superficial layer of the skin and what lies beneath it / there is white, gray or yellow fluid / there is an edge to the ulcer / there is a purulent discharge. Covering the skin/protecting it/moisturizing and healing ulcers/removing dead tissue/cleaning and treating infections/aiding healing.
Fourth degree : The presence of a deep ulcer that reaches from the surface layer of the skin to the muscles and bones. There is a foul odor. There is a brown or black secretion. There is a purulent secretion. Covering the skin / protecting it / moisturizing and healing ulcers / removing dead tissue / cleaning and treating infections / helping healing / filling the gap.
Precautions to be taken to prevent bed sores :
◼️ If the patient is bedridden, he must use an air-filled mattress (air mattress).
◼️ Use pillows between the joints (knees, elbows).
◼️ Use soft, clean and dry furniture.
◼️ Avoid forming folds in the bedding under the patient.
◼️ Monitor the skin constantly (dryness, wetness, redness).
◼️ Dry the body well after washing.
◼️ Eat balanced food.
◼️ Consult a physical therapist regarding appropriate exercises to improve blood circulation.
Ninth standard: Risk management and patient safety:
Risk management is the other side of patient safety and security. The risks that the patient may be exposed to in the hospital are identified, an analysis is made of them, and a method is developed for how to deal with them, solve them, and prevent them from occurring again.
· There are risks that come from people.
· Risks resulting from interventions to which patients are exposed.
· Risks from hospital infrastructure.
· Risks arising from the wrong work system.
Tenth Standard: Delivery and Receipt Policy:
The Purpose:
Communicating important information about patient care from one doctor to another, from one nurse to another, or from one person to another during the patient’s medical service shift.
Politics:
The commitment of the medical service providers during the work shift to provide and exchange general information about the patient while providing medical care to him. The head of the department develops a handover and receipt form that contains the important information that is exchanged between the medical service providers in his department. The medical service providers deliver and exchange medical information among themselves. During the work shift, according to the relevant guides and forms, information is exchanged between service providers during the exchange of work sessions, with sufficient time to discuss information about the patient and provide answers to inquiries about the care or service required to be provided to the patient. The head of the department ensures the continuous implementation of the handover and receipt process in the event of a transfer. The Patient Medical service providers exchange important information about the patient and provide answers to inquiries about the patient’s condition during the handover and handover process. The information that must be conveyed orally or through handover and handover forms is: the patient’s name, age, date of birth and address Diagnosis History Patients Allergies Medications/Food/Liquids Tests/ Tests, previous and planned operations, the patient’s health care plan within 24 hours, tests and analyzes required to be performed, procedures required before the patient is discharged.
Standard Eleven: Isolation and restriction policy
· The Patient Care Law guarantees the patient his right to enjoy his freedom and not be restricted or isolated in accordance with Article (36) of the law unless the emergency situation requires it. Isolation or restriction is an exceptional situation that the treatment team does not resort to as part of the treatment plan because the principle is to avoid them and use them after Exhausting the means that least restrict the patient's freedom.
· The patient's emergency situation is represented by the emergence of aggressive behavior or disturbed behavior that threatens his safety or the safety of others around him and constitutes an imminent danger that cannot be controlled or contained by means that are less restrictive of his freedom (such as reassuring the patient, using positive reinforcement, or modifying the environment surrounding him).
· Isolation and restriction procedures shall not be applied except by direct order from the responsible physician or his representative within the facility who has experience in applying these procedures.
· The therapeutic team performing the isolation or restraint must be professionally trained in both procedures and possess the skills that qualify it to carry out them, taking into account the application of internationally approved standards.
· Isolation or restriction procedures must be carried out according to methods that are psychologically and physically safe and preserve the patient’s dignity.
· Isolation or restriction measures must not be a means of coercion, discipline, comfort or retaliation by the treatment team.
· Isolation or restriction procedures shall be carried out for a specific time and must be terminated immediately upon the expiration of the reasons that necessitated their application, provided that the period of isolation or restriction for adults shall not exceed 8 continuous hours in accordance with the provisions of Article (36) of the executive regulations of the law, subject to renewal, but only after another debate and a new examination of the patient. By the responsible physician or his representative. Renewal requires the continuation of the emergency situation, and it is preferable that the time specified for the isolation or restriction procedure be in accordance with international standards as follows: -
o 4 hours for adults (18 years or older)
o 2 hours for teenagers (9-17 years old)
o One hour for children under 9 years old
· A patient subject to restraint or isolation reserves the right to see an official of the Patient Rights Committee and also has the right to file a complaint.
Isolation :is detaining the patient against his will in a room or area designated for that purpose, isolated from others, so that he cannot leave it, provided that the place conforms to all internationally approved specifications for isolation rooms.
Restriction :It is the restriction of the patient’s movement and its types:
Manual restraint: - Manually or physically, the patient is contained with the least amount of force by immobilizing his arms and legs, avoiding pressure on his back and neck, and keeping his position lying on his back as much as possible.
Mechanical restraint: What is meant is the use of tools or devices to limit the patient’s movement so that they are close to his body to the extent that he cannot easily escape from them. It also allows him little freedom of movement. It is safe and provides the patient with physical and psychological protection. It keeps the patient from falling. It is easy to adjust and does not waste dignity. For the patient, it does not require surgical intervention to install it. It allows for quick termination when an emergency occurs in the patient’s surroundings.
· When restraining, one person is required on each limb and another for the patient's head. The patient is placed lying on his back in the bed, and each ankle and wrist are tied so that he is tied to the bed from four sides. Soft restraints are used, such as gauze, leather restraints, or medical belts, according to the desired degree of fixation and the patient's condition, and are not applied. Restraints on the chest, neck and head.
To apply isolation or restriction measures, the following steps must be followed:
· Observation of the patient by the treatment team present with him in terms of behavior and actions and quickly predicting the presence of imminent danger as a result of his behavior.
· The treatment team (often the department's nursing staff) monitors any aggressive behavior in the patient or severe agitation that threatens his safety or the safety of others around him and evaluates it professionally, not personally, towards the patient.
· Trying to use the means that are least restrictive of the patient’s freedom, and after exhausting them and not being able to control the emergency situation, the treatment team resorts to containing the patient and trying to control his movement with physical restraint only. It is not permissible to isolate the patient or restrain him chemically or mechanically except by direct order from the responsible physician or his representative. .
· Fill out the paragraph related to the nursing staff member’s report on the emergency case in the isolation and restraint form
· Call the responsible doctor or his representative immediately to discuss the case and do the following:
o Clinical examination of the patient (psychologically and physically)
o Evaluate the extent of the risk and whether it requires the application of isolation or restraint measures, and attempts to control it by means that least restrict the patient’s freedom.
o Informing the patient of the reasons that necessitated isolation or restriction measures, the danger of his behavior to himself and others, and quickly ending the procedure if the reasons necessitating it do not exist.
· The responsible physician or his representative must complete the form for isolation and restraint, which includes:
o Clinical examination of the psychological and physical patient
o Risk aspects and severity
o Less restrictive means that have been exhausted
o The specified period of isolation or restriction
o The type of procedure that will be decided for the patient
o Description of the prescribed method of isolation or restraint, for example (the place of isolation is the patient’s room or another room - the mechanical restraint, the nature of the tools used in the procedure and how they are used and distributed among the parts of the body)
o Determine the start and end times of the procedure in isolation or restraint
o Pointing out the necessity of observing critically ill patients such that their condition requires special care, for example: patients with respiratory diseases, heart diseases, and patients with obesity and overweight.
o The responsible physician or his representative must state his name, signature, and the date of the procedure
o The procedure is performed under the direct supervision of the responsible or on-call physician and in the presence of one of them
o Identifying the cases and circumstances that require the treatment team to complete the procedure
o The responsible physician or his representative must review the patient’s treatment plan and update it according to the patient’s clinical condition and the circumstances surrounding him to avoid a recurrence of the emergency.
· A member of the therapeutic team is assigned to observe the patient face to face around the clock throughout the specified period of isolation or restriction, and to follow up on him every 15 minutes and record the following:
o Injuries that the patient may have suffered during the procedure
o Vital signs, respiratory rate, nutrition, skin color, behavior, and general condition
o Condition of blood circulation in the places of restriction (pulse, skin color)
o Movement rate, provided that restrictions are lifted every two hours for 10 minutes
o Provide him with fluids for two hours and record his intake
o The patient is given two hours of time to excrete (urine, stool) when needed
o It allows the patient to sleep and provides him with protection and comfort during sleep
o Ensure that restrictions are placed in their correct places and amend them when necessary
o Protecting the patient from others harming him (verbal and physical) during the procedure
o Observing the patient's ability to understand the procedure, his ability to adapt to it, and the form of his behavioral response
o The name of the nursing staff member performing the procedure and observation must be recorded on the isolation and restraint form
· The hospital is committed to creating a special record of isolation and restriction procedures, which records:
o Patient's name, registration number, admission date
o The type of procedure, its date, and its duration
o Name of the responsible physician and nursing staff member performing the procedure and observation
· The record is presented to the medical director daily, and the hospital administration is notified of this action immediately after it is taken during working hours or immediately the next morning when it is implemented in the shift.
Reasons for ending isolation or restriction measures:
· The signs of danger that necessitated applying the procedure have disappeared and the emergency situation has disappeared
· The success of one of the least restrictive means of the patient's freedom to control and modify the patient's behavior
· The appearance of signs of deterioration in the patient's organic condition requires terminating the procedure
· The occurrence of an emergency in the vicinity of the procedure that prevents its completion, such as a fire.