Benign paroxysmal positional vertigo (ECPG)
- Annexes
Editorial Independence:
▪️ This guideline was developed without any external funding.
▪️ All the guideline development group members have declared that they do not have any competing interests.
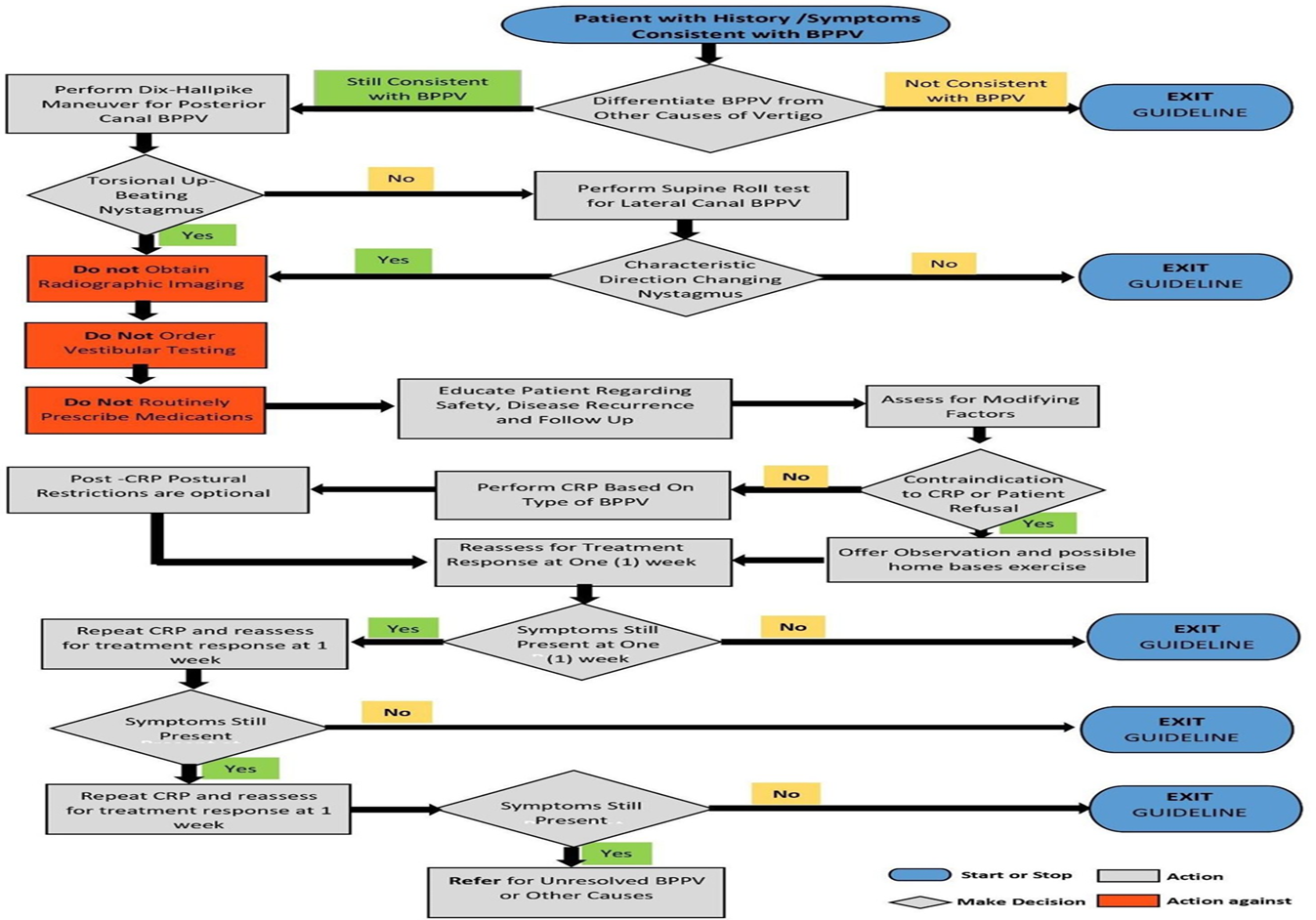
Annex 1: Guideline Flowchart
Annex 2: Tables of appraisal of selected guidelines: Currency (table 1), Content (table 2) and Quality (table 3) of the selected guidelines.
Table 1: Currency
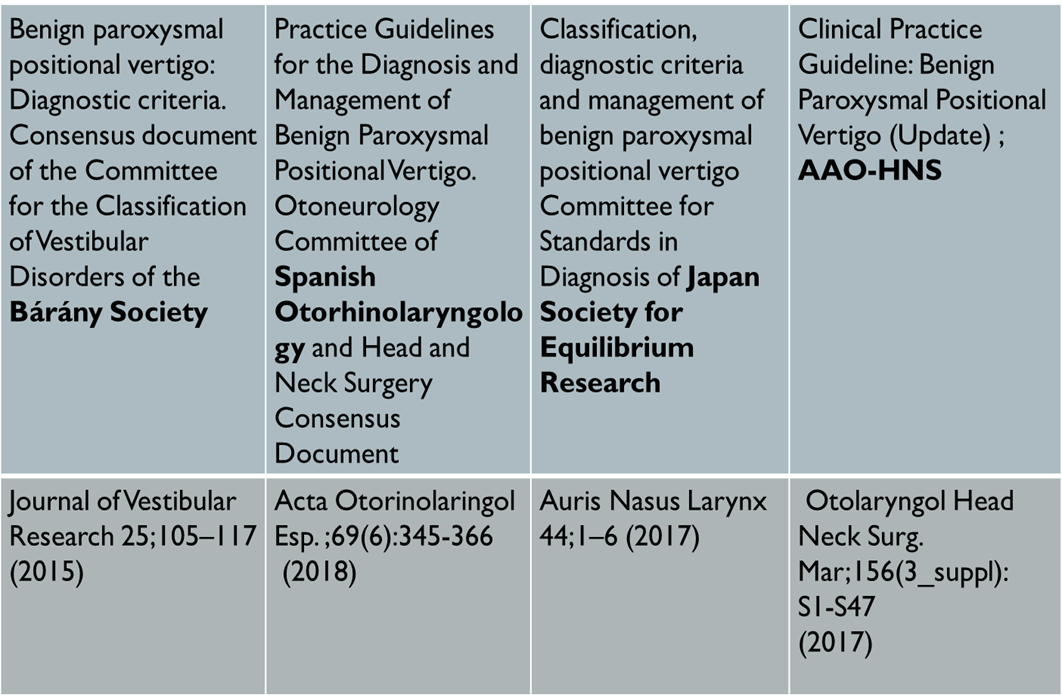
Table 2: Content
|
CRITERIA |
American Academy ORL-HNS |
Bárány Society |
Spanish ORL-HNS Consensus |
Japan Society for Equilibrium Research |
|
Credibility |
9/9 |
5.4/9 |
7.2/9 |
3.6/9 |
|
Observability |
9/9 |
7.2/9 |
3.6/9 |
3.6/9 |
|
Relevance |
9/9 |
7.2/9 |
7.2/9 |
5.4/9 |
|
Relative advantage |
7.2/9 |
7.2/9 |
7.2/9 |
7.2/9 |
|
Easy to install and understand |
9/9 |
9/9 |
7.2/9 |
5.4/9 |
|
Compatibility |
9/9 |
9/9 |
9/9 |
9/9 |
|
Testability |
9/9 |
9/9 |
9/9 |
9/9 |
|
Total |
61.2 |
54 |
50.4 |
43.2 |
Table 3: Quality
|
Domain |
AAO-HNS |
Bárány Society |
Spanish ORL- HNS Consensus |
Japan Society for Equilibrium Research |
|
1. Transparency |
A |
A |
C |
C |
|
2. Conflict of interest |
A |
A |
B |
B |
|
3. Development group |
A |
C |
C |
C |
|
4. Systematic review |
A |
B |
A |
B |
|
5. Grading of evidence |
A |
B |
B |
B |
|
6. Recommendations |
A |
C |
C |
C |
|
7. External review |
A |
A |
NR |
B |
|
8. Updating |
B |
B |
B |
B |
Annex 3: The risks and benefits of added and/or modified statements
|
Statement topic |
Original statement |
The statement action to be adapted |
Benefits |
Risk/Harm
|
|
Vestibular testing |
Clinicians should not order laboratory vestibular testing in a patient who meets diagnostic criteria for BPPV in the absence of additional vestibular signs and/or symptoms inconsistent with BPPV that warrant testing. |
Clinicians should not order laboratory vestibular testing in a patient who meets diagnostic criteria for BPPV in the absence of additional vestibular signs and/or symptoms inconsistent with BPPV that warrant testing. Vestibular testing may be ordered in case of recurrence, persistence of complaint after repositioning maneuver or in the presence of atypical nystagmus |
Diagnosis and treatment of possible causes of positional vertigo other than BPPV |
Cost of vestibular testing |
|
Repositioning procedures as initial therapy for posterior canal (a) |
Clinicians should treat, or refer to a clinician who can treat, patients with posterior canal BPPV with a canalith repositioning procedure |
Clinicians should treat, or refer to a clinician who can treat, patients with posterior canal BPPV with a canalith repositioning procedure. Epley or Semont are equivocally effective for post.canal BPPV |
High value ascribed to prompt resolution of symptoms and the ease with which the CRP may be performed |
No serious adverse events reported in controlled randomized trials |
|
Repositioning procedures as initial therapy for lateral canal (b) |
Not reported |
the barbecue roll maneuver or Gufoni maneuver appear moderately effective for the geotropic form of lateral semicircular canal BPPV |
Helps in resolution of patients symptoms |
None |
|
Post procedural restrictions |
Clinicians may not routinely recommend post procedural postural restrictions after canalith repositioning procedure for posterior canal BPPV. |
Clinicians may not routinely recommend post procedural postural restrictions after canalith repositioning procedure for posterior canal BPPV. Post procedural postrural restriction might be recommended in selected cases as in failure (or repeated failure) of the repositioning maneuvers, recurrent cases, or cases associated with other vestibular pathology as MD or vestibular Migraine. |
Help patients to tolerate symptoms till complete recovery |
Possible musculoskeletal discomfort and cost of cervical collars |
|
Number of CRP repetitions |
Not reported |
1-2 sessions would resolve the condition in 87-100% of patients. A minority would require a 3ed trial. Otherwise persistent BPPV is suspected. |
Help the clinician to search for causes of resolution failure |
Cost of investigations |
|
If there is difficulty in performing successful maneuver |
Not reported |
Clinicians should start with CRP (or modified) even in those patients who are very obese; have severe cervical or lumber discs; or upon patient’s preference. In the latter case patients should be instructed to avoid activities that may increase the risk of falls until symptoms resolve. |
Faster recovery and resolution of BPPV |
Patient discomfort and difficulty of performing the maneuver |
|
Observation as initial therapy
|
Clinicians may offer observation with follow up as initial management for patients with BPPV |
Clinicians may offer observation with follow up only if there is difficulty in performing successful maneuver after trials in some patients as : very obese; severe cervical or lumber discs; or upon patient's preference not to repeat the maneuver |
Avoidance of increased risks of falls; the use of vestibular suppressants with their known side effects |
Prolonged symptoms compared with other interventions that may expose patients to increased risks for falls or lost days of work; indirect costs of delayed resolution compared with other measures |
|
Vestibular rehabilitation |
The clinician may offer VR in the treatment of BPPV |
VR should be considered an option in the treatment of BPPV rather than a recommended first-line treatment modality. Home based Brandt-Daroff exercises is indicated in patients with persistent dizziness or imbalance after successful CRP or patients who refuse CRP.A more comprehensive customized VR program is indicated in patients with other vestibular pathology or with comorbid impairments that require balance rehabilitation specially in elderly. |
Reduce patient symptom in the mentioned cases |
None for home-based exercise. Cost if formal VR program is recommended |
|
Medical therapy |
Clinicians should not routinely treat BPPV with vestibular suppressant medications such as antihistamines and/or benzodiazepines |
Clinicians should not treat BPPV with vestibular suppressant medications such as antihistamines and/or benzodiazepines. Exceptions: Severely symptomatic patients refusing other treatment options and patients requiring prophylaxis for CRP |
Avoidance of adverse effects from, or medication interactions with, these medications; prevention of decreased diagnostic sensitivity from vestibular suppression during performance of the Dix-Hallpike maneuvers |
None |
|
Outcome assessment |
Clinicians should reassess patients within 1 month after an initial period of observation or treatment to document resolution or persistence of symptoms |
Clinicians should reassess patients within time frame of 3 weeks following the canalith repositioning procedure to document resolution, need for repetition of CRP session or persistence of symptoms |
Confirming the success of the maneuver; avoidance of missing other versions of BPPV as multiple canals or central causes |
None |