Pure-Tone Air-Conduction and Bone-Conduction Threshold Audiometry with and without Masking in Adults and Older Children (ECPG)
- Annexes
Editorial Independence:
● This guideline was developed without any external funding.
● All the guideline development group members have declared that they do not have any competing interests.
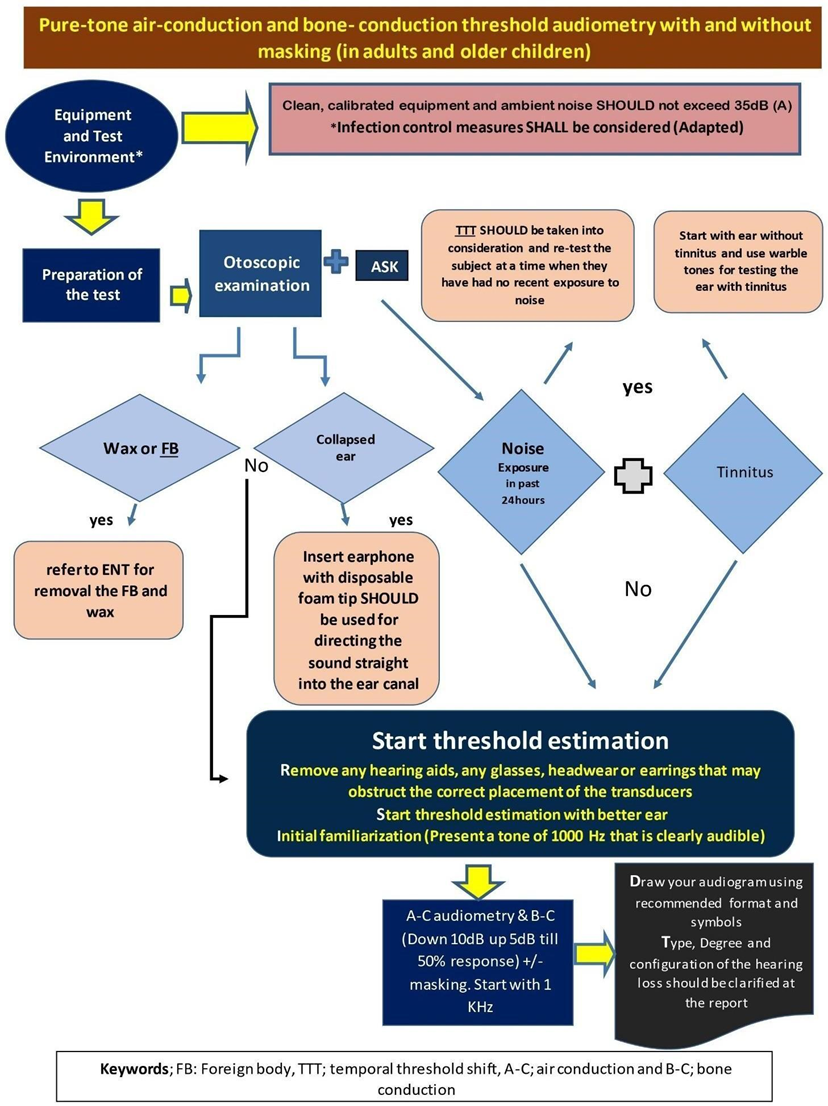
Annex 1: Guideline Flowchart
Annex 2: Tables of appraisal of selected guidelines: Currency (table 1), Content (table 2) and Quality (table 3) of the selected guidelines.
1.Assessment of Currency (table 1):
|
No |
Guideline name |
Organization |
Date of publication |
Date of review |
Age Demography |
|
1 |
Pure-tone air-conduction and bone- conduction threshold audiometry with and without masking |
British Society of Audiology |
January 2017 |
January 2022 |
Adult and old children |
|
2 |
Pure-tone air-conduction and bone- conduction threshold audiometry with and without masking |
British Society of Audiology |
August 2018 |
2023 |
Adult and old children |
|
3 |
ASHA 2005 |
American Speech-Language-Hearing Association (ASHA) |
2005 |
------- |
Adult |
|
4 |
French Society of ENT (SFORL) guidelines (short version): Audiometry in adults and children
|
French Society of ENT (SFORL) |
Jaunuary 2018 |
|
Adult and Children |
2- Assessment of Quality (Table 2)
|
Assessment of quality |
||||
|
Domain |
BSA 2017 |
BSA 2018 |
ASHA 2005 |
SFORL 2018 |
|
Transparency |
A |
A |
A |
A |
|
Conflict of interest |
B |
B |
B |
B |
|
Development group |
B |
B |
B |
B |
|
Systemic Review |
B |
B |
B |
C |
|
Grading of evidence |
D |
D |
B |
D |
|
Recommendation |
B |
B |
B |
B |
|
External Review |
A |
A |
A |
A |
|
Updating |
A |
A |
C |
B |
3- Content (Table 3)
|
Content |
||||
|
Criteria |
BSA2017 |
BSA2018 |
ASHA 2005 |
SFORL 2018 |
|
Credibility
|
IBSA 2011 9 |
BSA 2011 9 |
ANSI2004 9 |
7 |
|
Observability
|
9 |
9 |
8 |
5 |
|
Relevance
|
9 |
9 |
8 |
6 |
|
Relative Advantage |
9 |
8 |
7 |
6 |
|
Easy to install and understand |
9 |
9 |
7 |
7 |
|
Compatibility
|
9 |
9 |
7 |
6 |
|
Testability
|
9 |
9 |
9 |
6 |
|
Total |
63 |
62 |
55 |
43 |
Annex 3: The risks and benefits of added and/or modified statements.
|
Original statement |
The statement to be adapted: Action |
Benefits |
Risk/Harm |
|
||||||||||||||||||
|
1- 3000 and 6000 Hz may be required in cases of high frequency hearing loss
|
3000 and 6000 Hz should be done in all cases. |
Detection of v dips at these 2 frequencies facilitates early detection of suspected cases of retrocochlear lesions, very important in noise induced hearing loss, and in tinnitus patients. |
Increase the examination time. |
|
||||||||||||||||||
|
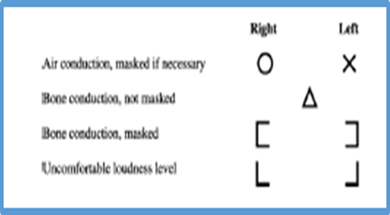
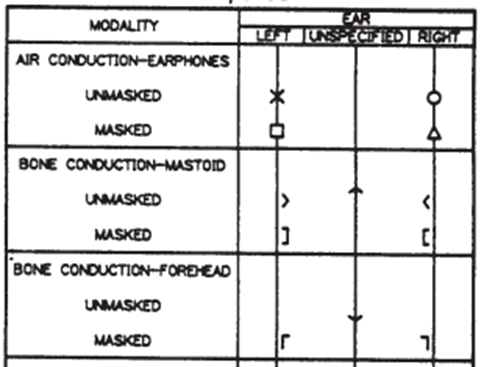
2- Audiometric symbols Not including the masked air conduction symbols
|
According to ASHS, 1990
|
The original in the document did not involve the masked air conduction symbols. |
No harm |
|
||||||||||||||||||
|
3- Audiometric descriptors and configurations
Four audiometric descriptors are given. These are based on the average of the pure-tone a-c hearing threshold levels at 250, 500, 1000, 2000 and 4000 Hz |
● Five audiometric descriptors are given According to ASHA, 2015 but in contrary to ASHA 2015, we adopt the average of pure tone hearing threshold at frequencies (250Hz, 500 Hz, 1KHz, 2KHz, and 4KHz) instead of 250Hz to 2KHz. ● We also clarify that as described previously by Northern and Downs (2002) that 15 dB HL as the upper limit for normal hearing for children between 2 and 18 years of age |
More precise and widely used |
No harm |
|
||||||||||||||||||
|
Averages do not imply any particular configuration of hearing loss and do not exclude additional terms (e.g. profound high-frequency hearing loss) being used.
|
The configuration, or shape, of the hearing loss refers to the degree and pattern of hearing loss across frequencies. For example, a hearing loss that only affects the high tones would be described as a high-frequency loss. On the other hand, if only the low frequencies were affected, the configuration would show poorer hearing for low tones and better hearing for high tones. Some hearing loss configurations are flat, indicating the same amount of hearing loss for low and high tones (ASHA, 2015). Moreover, if there is V dip at certain frequency, it should be described. We adapt the following table for the configuration description: quoted from Schlauch, R. S., & Nelson, P. B. (2009).
|
More precise and more informative.
|
No harm |
|
||||||||||||||||||
|
4- Guidelines of PTA in outbreaks: No statements were described in BSA as how to deal in highly infectious circumstances as in COVID 9 |
During The terrible COVID 19 outbreak, we adapt the American Academy Guidelines that were prescribed for vestibular testing during COVID with slight modification. |
Very beneficial to protect the health provider staff and also the personnel seeking the PTA |
Time consuming and costly. |
|