Pure-Tone Air-Conduction and Bone-Conduction Threshold Audiometry with and without Masking in Adults and Older Children (ECPG)
- Recommendations
The following statements and flowchart were adapted from the Guidelines from (The “Pure-tone air- conduction and bone-conduction threshold audiometry with and without masking” the recommended procedure by the British Society of Audiology BSA (2017)) which received the highest scores as regards the currency, contents, and quality.
Recommendations statements
|
Accepted statements |
|
|
Modified statements |
|
|
Added statements |
|



|
Statement topic |
Action recommendation |
Strength of recommendation according to BSA |
Evidence Quality |
Study Type |
References |
|
I. Equipment and test environment
|
Audiometer, transducers and response buttons SHALL be clean and regularly Calibrated (refer to section IX). |
Strong Recommendation |
Low |
Observational study |
[1] |
|
Ambient noise SHOULD not exceed the levels permitted (35dB (A)) measured by the sound level meter. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
|
The subject SHALL not be able to see or hear the tester adjust the audiometer controls. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
|
II. Preparation of the test subjects And full history taking
|
Audiometry SHALL be preceded by otoscopic examination. The findings recorded including the presence of wax and ear canal collapse. Occluding wax shall be removed prior to audiometry and use insert earphone in case of ear canal collapse. |
Strong Recommendation |
Very low |
Expert opinion |
[3] |
|
Subject SHALL be asked about any exposure to loud noise during the previous 24 hrs, as this can cause a temporary threshold shift. If the answer is yes, then more details should be obtained regarding the exposure and results recorded. Temporal threshold shift should be taken into consideration. It may be necessary to re-test the subject at a time when they have had no recent exposure to noise. |
Strong Recommendation |
Very low
|
Expert opinion |
[4]
|
|
|
Subjects SHALL be asked if they have tinnitus and if they have better hearing in one ear. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
|
III. Air-conduction audiometry
|
Remove any hearing aids, also any glasses, headwear or earrings that may obstruct the correct placement of the transducers, cause discomfort or affect sound transmission. Wherever possible, hair, scarves etc, SHOULD not be allowed to sit between the ear and the transducer. |
Conditional Recommendation |
Very low |
Expert opinion |
[3] |
|
Instructions: SHALL give clear information about the task. The patient responds to the faintest sound he/she hears. “Whatever the sound, and no matter how faint the sound, press the button as soon as you think you hear it, and release it as soon as you think it stops.” |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
|
Subject’s response * The subject’s response to the test tone SHOULD clearly indicate when the test tone is heard and when it is no longer heard. Response mode may be verbal, raising hands or push button. But the latter is the preferred method. Naïve patients may find it difficult to use push buttons. Alternatively, raising hand may be much easier. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
*When testing younger children, adults with learning difficulties or subjects with attention difficulties a more engaging response method may be required, and, if so, this SHALL be recorded. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
|
Earphones: Three main types of transducers can be used supra, circum aural or insert earphones The tester SHALL fit the earphones. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
|
The subject SHOULD be instructed not to hold them. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
The sound opening of the supra-aural earphones SHALL be aligned with the ear canal entrance. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |



|
III. Air-conduction audiometry
|
Test order Start with the better-hearing ear (according to the subject’s account) and at 1000 Hz. Next, test 2000 Hz, 4000 Hz, 8000 Hz, 500 Hz and 250 Hz in that order. Then, for the first ear only, retest at 1000 Hz. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
Mid frequencies may be required in presence of > 20dB difference between two adjacent octave frequencies in frequency range (250-8000 Hz) (Modified from ASHA 2005). |
Conditional recommendation |
Very low |
Expert opinion |
[5] |
|
|
Testing 3000 Hz and 6000 Hz may be required in cases of high- frequency hearing loss, tinnitus and suspicion of retro- cochlear pathology |
Conditional recommendation |
Very low |
Expert opinion |
[5] |
|
|
Timing of the test stimuli: The duration of the presented tone shall be varied between 1 and 3 seconds. The interval between the tones shall be varied between 1 sec. and at least 3 seconds. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
Initial familiarization Present a tone of 1000 Hz that is clearly audible (e.g. at 40 dB HL for a normally hearing subject or approximately 30 dB above the estimated threshold for a subject with a hearing impairment, but never more than 80 dB HL). If there is no response, increase in 10-dB steps until a response occurs. If the tone is still inaudible at 80 dB HL, increase 5-dB steps until a response occurs, taking care to monitor the subject for discomfort. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
Method for finding threshold 1. Following a satisfactory positive response, reduce the level of the tone in 10-dB steps until no further response occurs. 2. Increase the level of the tone in 5-dB steps until a response occurs. 3. After the first response using an ascending approach, decrease the level by 10 dB and begin another ascending 5-dB series until the subject responds 4. Again decrease the level by 10 dB and increase by 5 dB until the subject responds at the same level on two out of two, three or four (i.e. 50 % or more) responses on the ascent. This is the hearing threshold level. Proceed to the next frequency, starting at a clearly audible level (e.g. 30 dB above the adjacent threshold). |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
IV. Variants in methods
|
1. Industrial audiometry: requires testing at 500 Hz, 1000 Hz, 2000 Hz, 3000 Hz, 4000 Hz, 6000 Hz and 8000 Hz. 2. Subjects with short attention spans, and some elderly subjects: in these cases, it may be appropriate to test fewer frequencies with use of longer test tones or alternative response methods. 3. Subjects with tinnitus: If the subject is unable to perform an accurate test at some frequencies due to an inability to distinguish between their tinnitus and the test tone, then a frequency-modulated or warble tone may be used as a stimulus. The use of pulsed tones and narrow-band noise is not advised due to calibration and perception problems. 4. Exaggerated thresholds: published variations in technique may help with this (e.g. Cooper & Lightfoot, 2000). |
Strong recommendation |
Very low
Low |
Expert opinion
Observational study |
[2]
[6]
|
|
|
5. Ascending technique may be adopted in certain patients, such as non-organic HL, elderly and inattentive. |
|
Low, very low |
Observationa study + expert opinion |
[5, 6]
|
|
|
Variations in technique SHALL be recorded. |
|
Very low |
Expert opinion |
[2] |







|
Statement topic |
Action recommendation |
Strength of recommendation according to BSA |
Evidence Quality |
Study Type |
References |
|
V. Bone conduction audiometry
|
The bone vibrator is normally initially placed over the mastoid prominence of the worse hearing ear (as defined by the a-c thresholds averaged between 500 Hz and 4000 Hz), with the required area of the vibrator in contact with the skull. It SHALL be placed as near as possible behind the pinna without touching it and without resting on hair. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
The vibrator SHALL be held firmly in place by means of a headband that holds it against the skull with the required static force. |
Strong Recommendation |
Very low |
Expert opinion |
[2] |
|
|
The procedure is similar to the AC audiometry. The canal MUST NOT be occluded at test frequencies below 3000 Hz, as this may artificially improve b-c thresholds due to the ’occlusion effect ‘. Tested ear SHOULD be occluded with ear plug when testing 4000 Hz b-c. |
Conditional recommendation |
Low
|
Observation studies |
[7-12]
|
|
|
Narrow Band Masking noise SHOULD be used. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
VI. Masking
|
Cross-hearing and masking Rule 1 Masking is needed at any frequency where the difference between the left and right not-masked a-c thresholds is 40 dB or more when using supra- or circum-aural earphones or 55 dB when using insert earphones. Rule 2 Masking is needed at any frequency where the not-masked b-c threshold is better than the air-conduction threshold of either ear by 10 dB or more. Rule 3 Masking will be needed where the b-c threshold of one ear is more acute by 40 dB or more (if supra or circum-aural earphones have been used) or 55 dB or more (if insert earphones have been used) than the not-masked a-c threshold attributed to the other ear. |
Conditional recommendation |
Low |
Observational study |
[13]
|
|
Procedure for masking: (Plateau-seeking method for masking). Re-establish hearing threshold in the test ear by presenting the tone and seeking the response without masking noise to remind the subject what to listen for. Introduce masking noise to the non-test ear. The initial level of masking SHOULD be the effective masking level which is equal to the tonal threshold level of that ear at that frequency. using increments of 10 dB in masking noise, until you have at least four measurements (including the initial starting point) and until three successive measurements yield the same tonal threshold. You may be unable to obtain this plateau due to maximum level of the audiometer being reached or because the subject finds the masking noise uncomfortable. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |


|
Statement topic |
Action recommendation |
Strength of recommendation according to BSA |
Evidence Quality |
Study Type |
References |
|
|
Masking during bone-conduction testing: -An insert earphone SHOULD be used to deliver masking noise to the non-test ear for b-c testing, for subject comfort and for the advantages of high transcranial transmission loss, measurements yield the same tonal threshold. A supra-aural or circumaural earphone can be used if there is no alternative. -You may be unable to obtain this plateau due to maximum level of the audiometer being reached or because the subject finds the masking noise uncomfortable; in either case mark as unreached. -When three successive levels of masking yield the same tonal threshold, or one threshold is no more than 5 dB different from the other two, this is the ‘plateau’. The mode (i.e. the threshold which occurs 2/3) of the three hearing threshold levels at plateau is taken as the correct hearing threshold of the test ear and no further masking is required. Withdraw the masking noise and plot the hearing threshold level on the audiogram. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
-In subjects with tinnitus and hyperacusis, extra care SHOULD be taken when using high levels of masking noise, as this can exacerbate the tinnitus and worsen hyperacusis. In some cases, it may be appropriate not to perform masking |
Conditional recommendation |
Very low |
Expert opinion |
[4] |
|
|
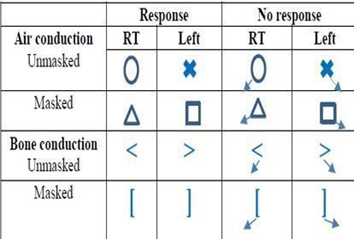
VII. Recommended format and symbols
|
• Hearing threshold level can be plotted graphically on an audiogram form. The aspect ratio SHOULD be fixed at 20 dB:1 octave in all cases to ease interpretation. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
• Air-conduction symbols SHOULD be connected with continuous straight lines; bone-conduction symbols SHOULD be joined with broken lines. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
• If no response occurs at the maximum output level of the audiometer, a downward arrow SHOULD be drawn, attached to the corner of the appropriate symbol. These symbols SHOULD not be connected with the line to symbols representing measured thresholds. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
(ASHA, 1990)
|
Conditional recommendation |
Very low |
Expert opinion |
[14] |




|
Statement topic |
Action recommendation |
Strength of recommendation according to BSA |
Evidence Quality |
Study Type |
References |
|
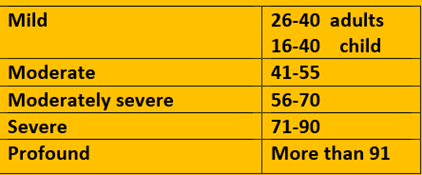
VIII. Descriptor Average hearing threshold levels (dB HL)
|
Descriptor Average hearing threshold levels (dB HL) (ASHA, 2015). These are based on the average of pure tone hearing threshold at frequencies (250Hz, 500 Hz, 1KHz, 2 KHz and 4KHz).
We also clarify that as described previously by Northern and Downs (2002) that 15 dB HL as the upper limit for normal hearing for children between 2 and 18 years of age. |
Conditional recommendation |
Low |
Observational study |
[15-17] |
|
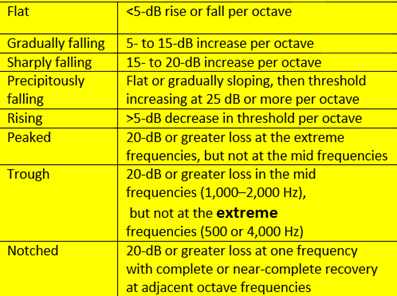
b) Report SHOULD illustrate (Type, Degree and configuration) of the hearing loss. There are three basic types of hearing loss: conductive, sensorineural hearing loss (SNHL), and mixed (ASHA, 2005). The configuration, or shape, of the hearing loss refers to the degree and pattern of hearing loss across frequencies. For example, a hearing loss that only affects the high tones would be described as a high-frequency loss. On the other hand, if only the low frequencies were affected, the configuration would show poorer hearing for low tones and better hearing for high tones. Some hearing loss configurations are flat, indicating the same amount of hearing loss for low and high tones (ASHA, 2015). Moreover, if there is V dip at certain frequency, it SHOULD be described. |
Conditional recommendation |
Very low |
Expert opinion |
[5, 15] |
|
|
Quoted from Schlauch, R. S., & Nelson, P. B. (2009)
|
Conditional recommendation |
Very low
|
Expert opinion |
[17] |
|
|
|
For the purposes of this document, in determining the five- frequency average value of hearing loss, if at any frequency no response is obtained due to the severity of the loss, this reading SHALL be given a value of 130 dB HL. Any hearing threshold level lower (better) than 0 dB HL SHALL be given the value 0 dB HL. |
Strong recommendation |
Very low |
Expert opinion |
[2] |



|
Statement topic |
Action recommendation |
Strength of recommendation according to BSA |
Evidence Quality |
Study Type |
References |
|
IX. Calibration
|
Stage A: routine checking and subjective tests: SHOULD be carried out in daily and weekly manner. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
Stage B: periodic objective tests are objective tests which ideally SHOULD be performed every 3 months. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
Stage C: basic calibration tests They will only be required when a serious error or fault occurs, or when, after a long period of time, it is suspected that the equipment may no longer be performing fully to specifications. It may be advisable to submit equipment for a Stage C check after, for example, five years’ use if it has not received such a test in that time in the course of repair. |
Conditional recommendation |
Very low |
Expert opinion |
[2] |
|
|
X. Guidelines of PTA in outbreaks:
|
During The terrible COVID 19 outbreak, we adapt the Guidelines that were published with AIHHP, BAA, BSA & BSHAA , 2021 updated June 2021. The following are the main points that should be followed during the pandemics: Apply triage system to determine which patient will be suitable for face to face appointment A) Questions you should ask to triage for Covid-19 symptoms Do you or anyone in your household/bubble: I. have coronavirus? II. have a new continuous cough? III. have a high temperature (37.8oC or over?) IV. have a loss or change in your sense of smell or taste? V. Have you or any member of your household/bubble been told to self-isolate after travel from a high-risk country or contact from test and trace? B) During an appointment the following must be observed: • Best practice hand hygiene • The use of Type II R facemasks for staff and patients (if tolerated) is required. • Physical Distancing of 2 meters remains best practice unless providing clinical care. If this is not possible the use of physical barriers as agreed with local infection prevention should be considered. • Best Practice respiratory hygiene (‘catch it, bin it, kill it’) and avoiding touching your face with your hands is required. C) After an appointment the following should be observed: • Leave enough time to doff any PPE, to clean high touch areas a patient has been in contact with, and to prepare for the next patient. No statements were described in BSA, 2017 as how to deal in highly infectious circumstances as in COVID 19. |
Conditional recommendation |
Very low |
Expert opinion |
[18] |

