Dysarthria (ECPG)
- Annexes
Editorial Independence:
- This guideline was developed without any external funding.
- All the guideline development group members have declared that they do not have any competing interests.

Annex2 :
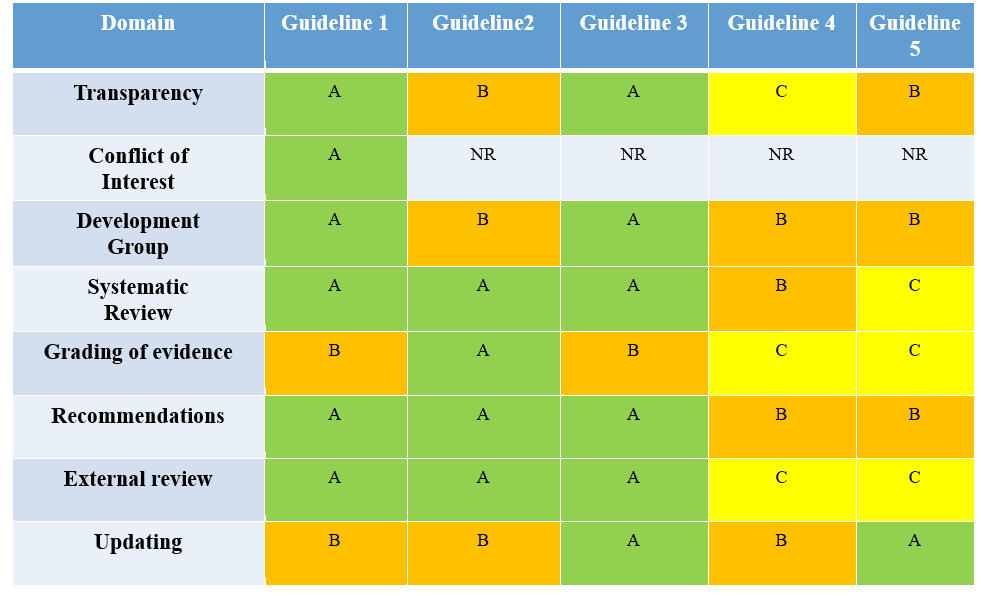
Tables of appraisal of selected guidelines: Currency (table 1), Content (table 2) and Quality (table 3) of the selected guidelines.
Table 1: Currency
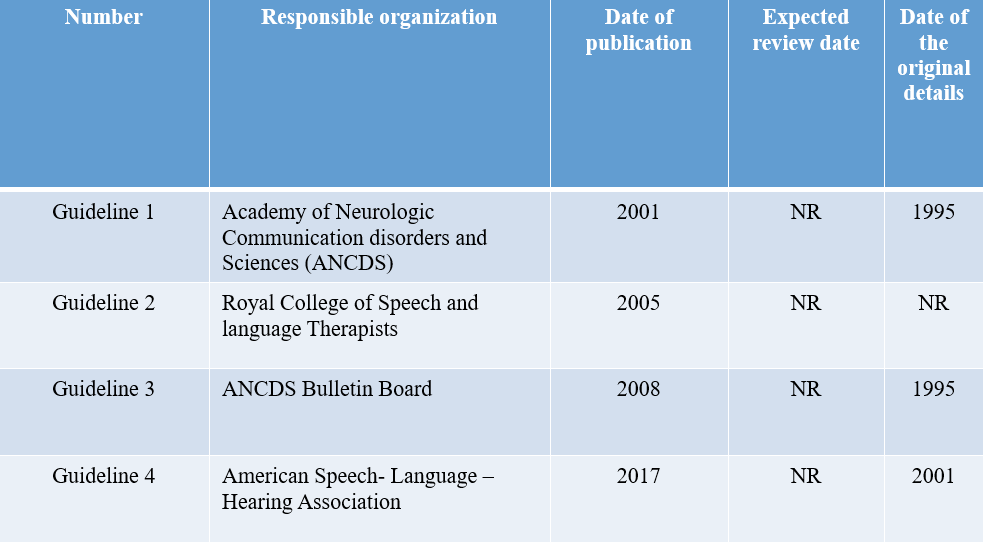
Table 2: Content
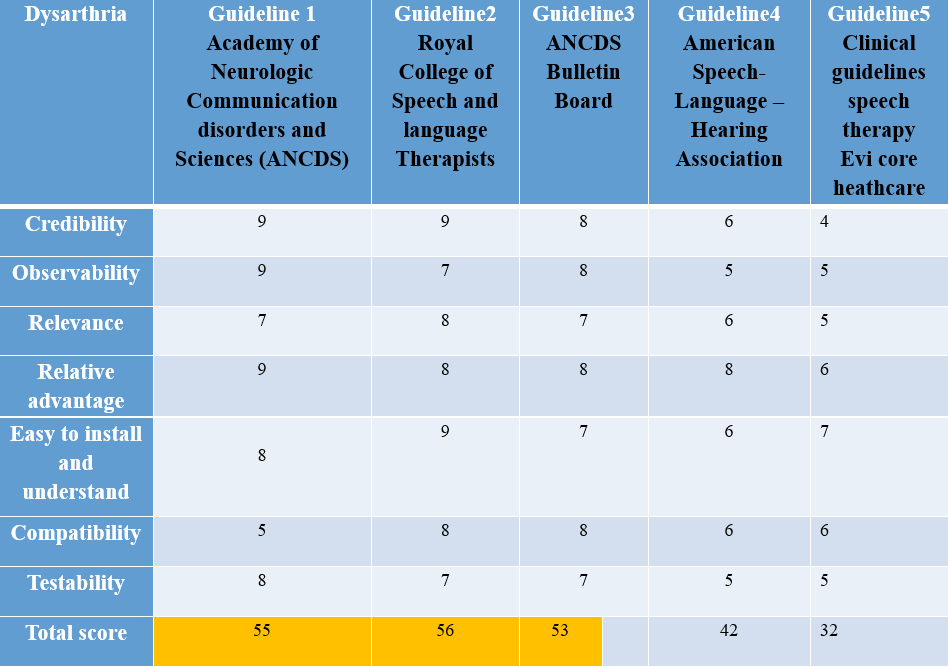
Table 3: Quality
Annex 3:
The risks and benefit from added or modified statements
|
Statement |
Risk |
benefit |
|
Smith accent voice therapy technique will improve function of respiration and phonation in the form of: § Increase loudness. § Better respiratory support. § Slowing the rate of speech. Adjust onset of phonation and respiration. |
May not applied by all physicians. It is usually known and applied by middle east physicians |
Mandatory in cases of dysarthria as it corrects the prosodic affection as well as loudness and respiratory incoordination and hence improve intelligibility |
|
Treatment of articulatory errors using: Consonant exaggeration. Syllable by syllable attack. Slowing the rate of speech. Oral muscular exercises are not mandatory for weak musculature as muscle tone needed for speech is different from muscle tone needed for the swallowing process.
|
Speech Intelligibility won’t improve |
Essential to improve speech intelligibility |
|
Therapeutic intervention for: Pitch inflections, stress and tone units |
The tone of speech as well as other prosody elements still affected with abnormal speech performance |
Prosodic correction |
|
Augmentative and alternative communication in case of: *Failed traditional therapy. *Anarthria. |
May stop trying to train verbal communication |
There is need to train patients using AAC to overcome loss of communication in cases of anarthria |
|
Good prognosis with: Young age. Early intervention. Intensive therapeutic strategies. |
Unrealistic expectations might stop commitment to therapy intervention |
Adding prognostic apects may motivate patients and caregivers to continue therapy even if slow improvement is seen |